MP63-05: Outcomes in Patients (Pts) With Bacillus Calmette-Guerin (BCG)-Unresponsive High-Risk (HR) Non-Muscle-Invasive Bladder Cancer (NMIBC) Who Underwent Radical Cystectomy (RC) Following Pembrolizumab (Pembro) Treatment in KEYNOTE-057 Cohort A
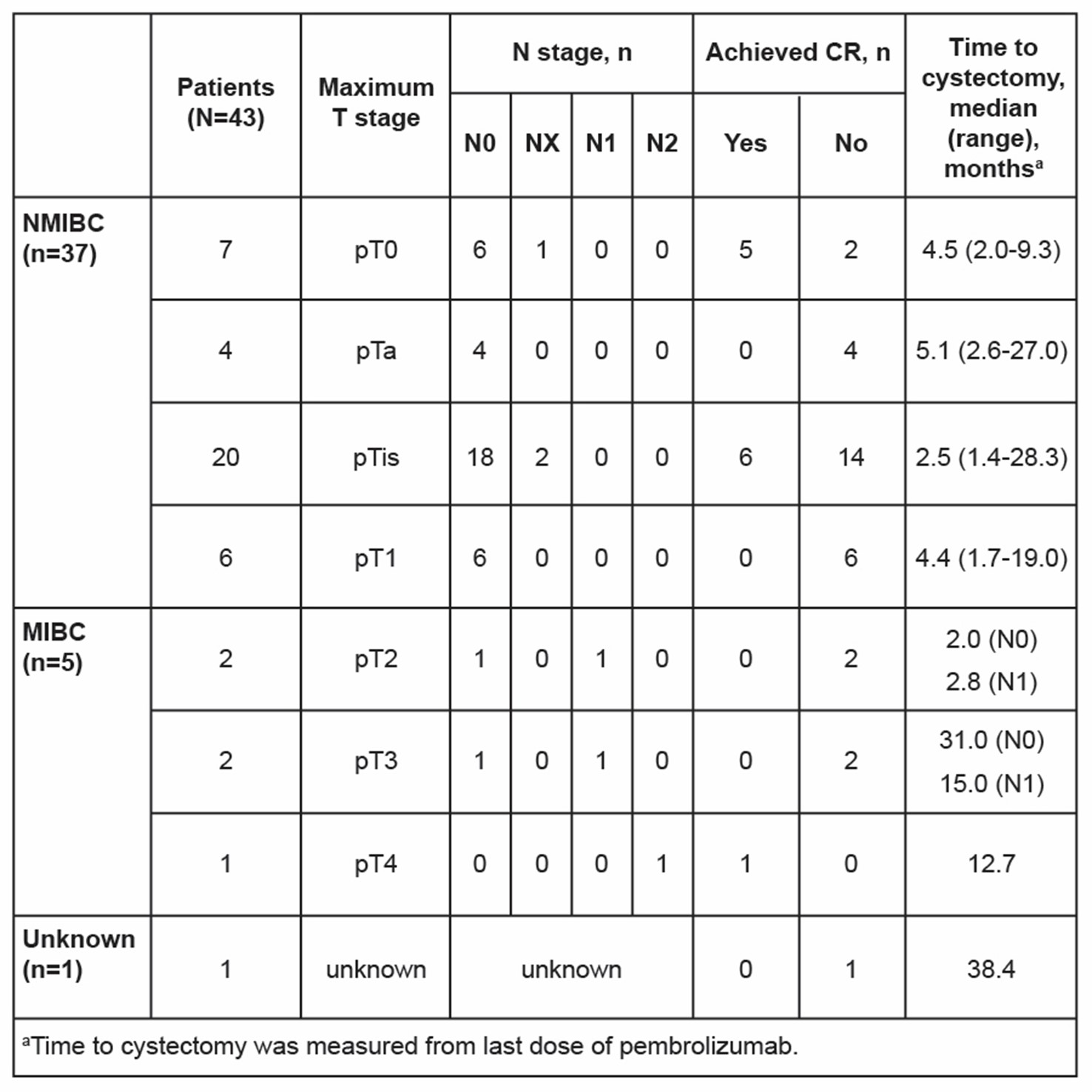
Introduction: Cohort A of KEYNOTE-057 (NCT02625961) showed durable antitumor activity and manageable toxicity with pembro in pts with BCG-unresponsive HR NMIBC with carcinoma in situ (CIS) ± papillary disease. We explored outcomes of pts in KEYNOTE-057 cohort A who underwent RC after discontinuing pembro. Methods: Eligible adults with histologically confirmed BCG-unresponsive HR NMIBC with CIS +/- high-grade Ta or T1 tumor and predominantly urothelial histology who were ineligible for or declined RC received pembro 200 mg IV Q3W for =2 yrs. Primary end point: complete response (CR) rate; secondary end point was DOR. Cystectomy-free survival (CFS), calculated from first dose of pembro, was evaluated in all pts to compare CFS between complete responders vs non–complete responders. Time to cystectomy and pathologic staging at time of RC were evaluated. Results: As of May 25, 2022, median follow-up for 96 enrolled pts was 60.4 mo (range, 50.2-72.5). CR rate was 41% (n=39) at 3 mo, and median DOR was 16.2 mo (range, 0.0+ to 57.7+). Median CFS was 56.8 mo (95% CI, 30.9-NR) for pts with CR and 18.5 mo (95% CI, 7.8-36.5) for pts without CR. Out of 96 enrolled pts, 43 underwent RC after discontinuing pembro (12 with initial CR followed by recurrence/progression and 31 without CR). Median time to RC from first dose of pembro was 9.0 mo (range, 4.0-41.8) for all pts who underwent RC, 14.3 mo (range, 9.0-32.5) for pts with initial CR, and 6.4 mo (range, 4.0-41.8) for pts without CR. Pathologic staging results are presented (table). Of 43 pts who underwent RC, 5 (12%) had upstaging to MIBC, of whom 4 never achieved CR and 1 achieved initial CR. Pts who developed =pT3 disease underwent RC >1 year after last dose of pembro. Conclusions: This exploratory analysis suggests that pembro may result in a clinically meaningful delay in RC in pts with BCG-unresponsive HR NMIBC with CIS, especially in pts who achieve an initial CR. Rates of upstaging at time of RC among pts who do not achieve a CR with pembro are generally consistent with previous reports of pts who undergo immediate RC, suggesting that the window of opportunity for subsequent RC is largely preserved. SOURCE OF Funding: Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA