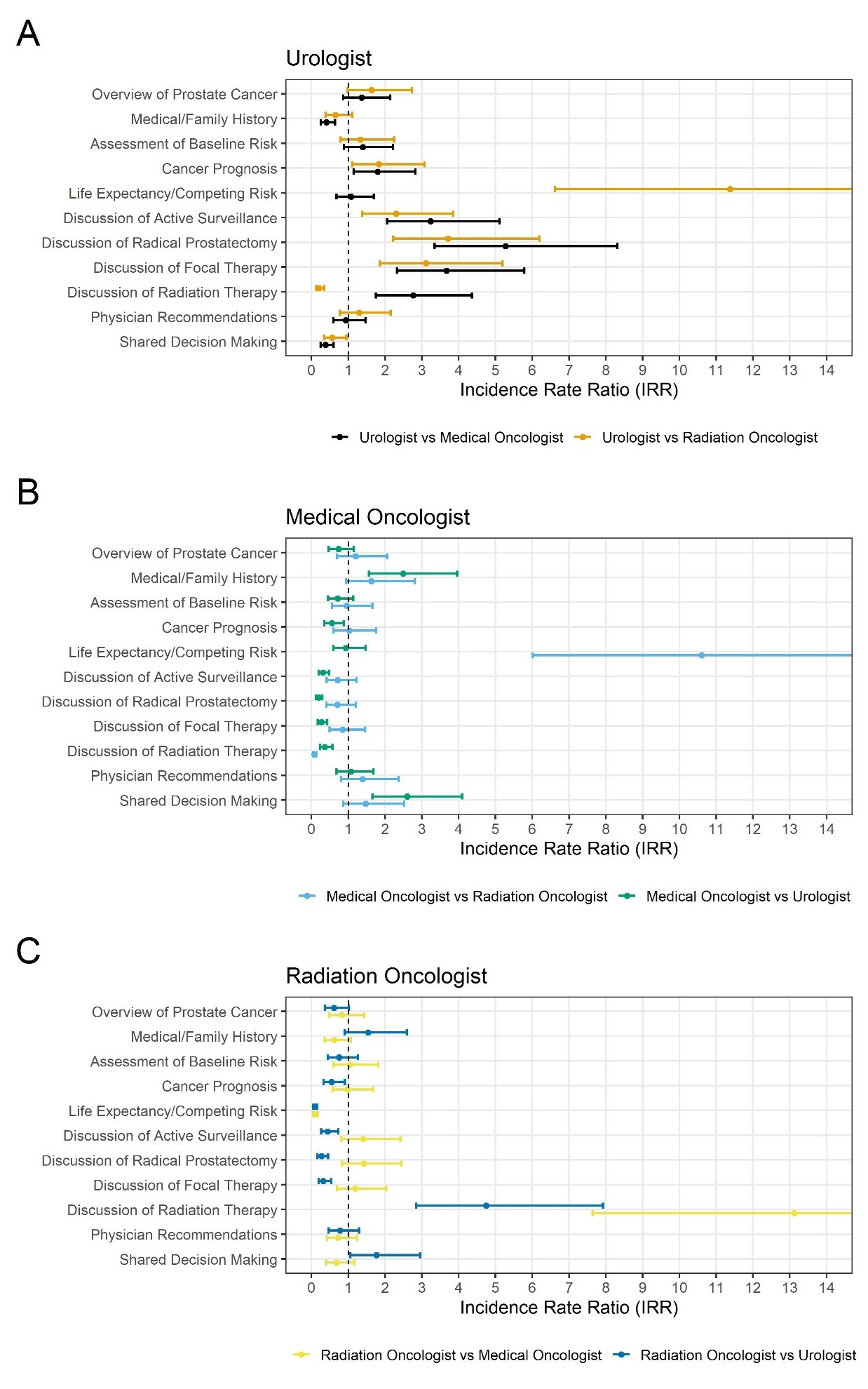
Introduction: Patients often consult with Urology, Radiation Oncology, and Medical Oncology when considering treatment options for prostate cancer. However, it is unknown what content each specialty discusses during consultations. Methods: We transcribed consultations of men with localized prostate cancer across 3 urologists, 3 radiation oncologists, and 3 medical oncologists. Coders independently coded consultations for narrative content. Reviewers identified 11 content areas: Overview of prostate cancer; medical history; assessment of baseline risk; cancer prognosis; life expectancy/competing risks; discussion of active surveillance, radical prostatectomy, focal therapy, and radiation therapy; physician recommendations; and shared decision making (SDM). We then calculated the number of words devoted to each content area per consult as a proxy for time spent. We then compared incidence rate ratio (IRR) for content-specific word count across specialties using a multivariable Poisson regression. Results: Our analytic sample included 5,569 segments of conversation across 28 Urology, 11 Radiation Oncology, 11 Medical Oncology consultations. In addition to spending more time discussing surgical treatments, Urologists also spent 1.8-fold more time discussing cancer prognosis than both Medical Oncologists and Radiation Oncologists (p < 0.03 for both). Urologists also spent 11-fold more time discussing competing risks than Radiation Oncologists (p < 0.0001). Medical Oncologists devoted 2.6-fold more time on SDM than Urologists (p < 0.0001). Medical Oncologists spent 10-fold more time discussing life expectancy/competing risks than Radiation Oncologists (p < 0.0001). In additional to spending more time discussing radiation therapy, Radiation Oncologists spent 1.7-fold more time on SDM than Urologists (p < 0.04). Conclusions: Multidisciplinary specialists focus effort on different areas of content in consultations, beyond the specific treatments they offer. Urologists appear to more thoroughly discuss prognosis than other specialists but spend the least amount of time on SDM. SOURCE OF Funding: Dr. Daskivich is supported by career development award CA230155 from the NIH/NCI. Dr. Friedrich was funded by NIH grant T32CA240172-03