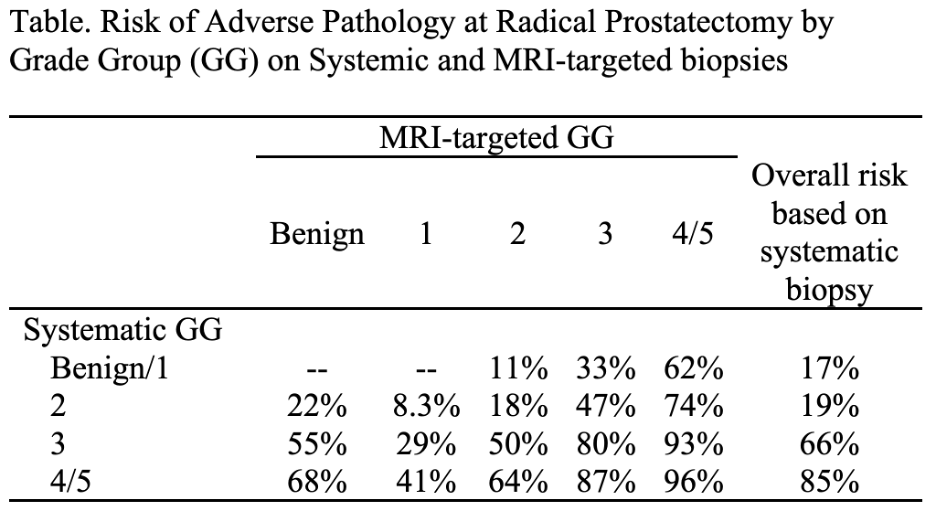
Introduction: MRI-targeted prostate biopsy (MR-Bx) in combination with systemic biopsy (S-Bx) improves detection of higher grade group (GG) prostate cancer compared to either modality alone. However, prognostic models using GG rely on pre-MRI era data; it is unknown whether upgrading with MRI-targeted cores portends increased oncologic risk or if this precise targeting and increased sampling is causing grade migration. We sought to define the relative oncologic risk of systematic and MRI-targeted biopsy cores in men treated with radical prostatectomy (RP) as defined by adverse pathology (AP) and biochemical recurrence (BCR). Methods: We retrospectively reviewed all patients who had MR-Bx and S-Bx prior to RP (2014-2022). We created two multivariable logistic regression models with AP (defined as primary pattern 4, any pattern 5, SVI or LNI) as the primary outcome. Pre-RP PSA, positive cores on S-Bx, negative cores on S-Bx, GG on S-Bx, and GG on MR-Bx. The second model excluded GG on MR-Bx. We derived the risk of AP for an average patient based on each combination of GG on S-Bx and MR-Bx in the first model and the risk of AP based on S-Bx GG in the second. As a secondary analysis, we used Cox instead of logistic regression for the outcome of BCR and presented risk at 12-months. Results: We identified 991 patients (median age 64) evaluated with MR-Bx and S-Bx and treated with RP. 359 (36%) had AP. MR-Bx GG portends additional risk compared to S-Bx GG alone (p < 0.001) but confers less risk than S-Bx of the same GG. The risk of AP is greatest when the highest GG is concordant between MR-Bx and S-Bx compared to when the highest GG is found on S-Bx or MR-Bx alone. For example, the risk of AP for GG2 S-Bx / GG2 MR-Bx, GG2 S-Bx / GG3 MR-Bx, GG3 S-Bx / GG2 MR-Bx, and GG3 S-Bx / GG3 MR-Bx are 18%, 47%, 50% and 80% respectively (Table). 158 patients experienced BCR. Results for the outcome of BCR were like those for AP. Conclusions: Where grade is discordant between systematic and MRI-targeted biopsy, risk is intermediate between the two grades. This casts doubt on the current practice of defining pathologic risk based on the highest grade. Prospective multicenter studies are required to accrue samples sizes large enough to estimate risk separately for all combinations of MRI and systematic grade. SOURCE OF Funding: N/A