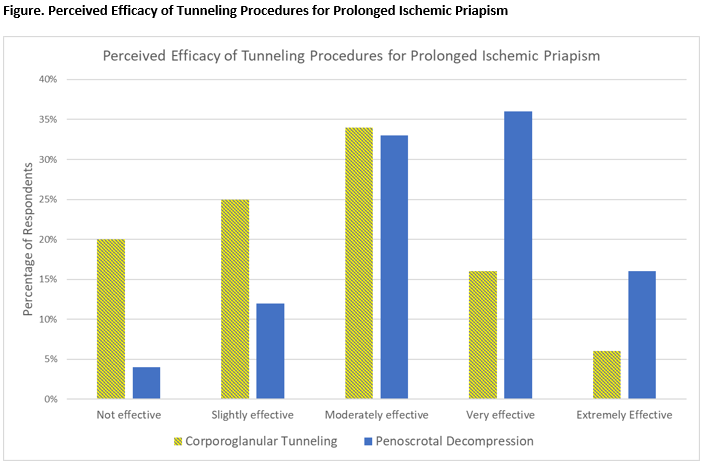
Introduction: Prolonged ischemic priapism (PIP) presents a rare and challenging urological condition, often requiring advanced surgical maneuvers for resolution. We sought to evaluate current practice patterns in the management of this challenging condition using a multi-institutional survey. Methods: A 38-question, web-based survey was distributed to clinically active urologic surgeons including members of the Society of Genitourinary Reconstructive Surgeons (GURS) and the Sexual Medicine Society of North America (SMSNA). PIP was defined as priapism duration of at least 24 hours prior to presentation. Questions highlighted experience with and perceived efficacy of adjunctive maneuvers including distal shunting, corporoglanular tunneling (CGT) and penoscrotal decompression (PSD). Also queried were surgeons’ impressions of the prevalence of erectile dysfunction after priapism surgery. Results: One hundred fifteen responses were received following survey distribution. Tunneling procedures (CGT and PSD) were the favored first-line intervention for PIP over implants (80/114 tunneling vs. 11/114 implant, p < .001). Respondents were more likely to have performed CGT than PSD (110/113 for CGT vs. 74/112 for PSD, p < .001), but among those who had performed both, PSD was felt to be more than twice as effective at resolving PIP (33/63, 52% Very or Extremely Effective for PSD, vs. 13/64, 20% for CGT; p < .001, Figure). For patients with recurrent priapism after CGT, PSD was the preferred salvage procedure for 46% of surgeons (46/99) while immediate implant was favored by 40% (40/99, p = .390). Regarding sexual function, a similar number of respondents who had performed both tunneling procedures felt that at least half of patients regained adequate sexual function after either CGT or PSD (27/61, 44% vs. 25/60, 42%; p = .773). Conclusions: PSD is perceived by surgeons as more effective than CGT for prolonged ischemic priapism and is commonly chosen as a salvage procedure when CGT fails. Many surgeons feel that patients regain erectile function after tunneling procedures, avoiding the need for expensive prosthetics. SOURCE OF Funding: N/A