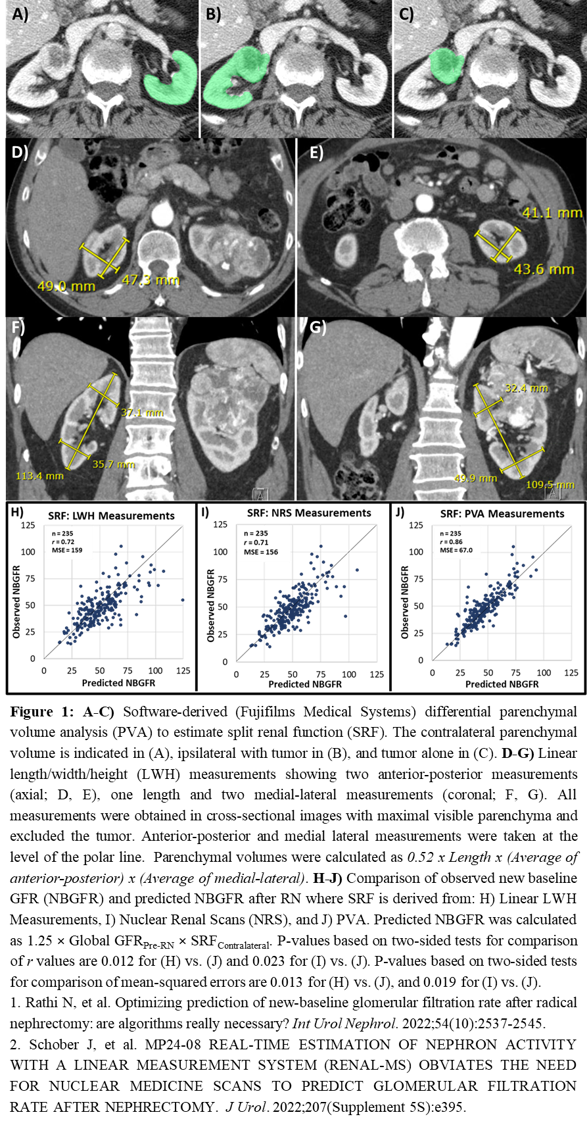
Introduction: While radical nephrectomy (RN) is an important consideration for renal tumors with increased complexity and oncologic potential, reduced postoperative new baseline GFR (NBGFR) relative to partial nephrectomy (PN) remains a concern. Thus, accurate predictions of NBGFR after RN can have clinical implications for RCC management, particularly in challenging cases where RN/PN offer distinct merits. Preoperative global GFR, split renal function (SRF), and renal functional compensation (RFC) in the contralateral kidney have been shown to be fundamental parameters for the accurate prediction of NBGFR after RN. While SRF has traditionally been obtained from nuclear renal scans (NRS), recent studies suggest that software-derived differential parenchymal volume analysis (PVA) is more accurate.1 A simplified approach to estimate SRF based on linear length/width/height measurements (LWH) has also been proposed.2 In this study, we compare the accuracies of each of these three methods for determining SRF, and, by extension, predicting NBGFR. Methods: All 235 RCC patients managed with RN (2006-21) with preoperative CT/MRI, NRS, and preoperative and postoperative GFR data were included. PVA was performed on CT/MRI using a 3D imaging software (Figure 1A-C), and LWH (Figure 1D-G) measurements were obtained using basic tools in the CT/MRI user interface. NBGFR was defined as the GFR 3-12 months after RN, and RFC was approximated at 25% based on prior studies (Predicted NBGFR = 1.25 × Global GFRPre-RN × SRFContralateral). Predictive accuracies were assessed by correlation coefficients (r) and mean-squared errors. Results: The r values for the LWH-, NRS-, and PVA-based approaches were 0.72, 0.71, and 0.86, respectively (Figure 1H-J). Differences in predictive accuracies of the PVA-based and non-PVA-based approaches were statistically significant. Conclusions: Software-derived PVA provides the most precise and accurate estimations of SRF, and thus NBGFR after RN, when compared to NRS and LWH methods. Clinically, the PVA-based approach can readily provide accurate predictions of NBGFR in challenging RCC cases where RN is a relevant consideration. Furthermore, the LWH approach, which can also be performed at point of care, is equivalent to NRS, precluding the need for NRS in most patients. SOURCE OF Funding: N/A

.jpg "Nityam Rathi, BS (he/him/his) photo")