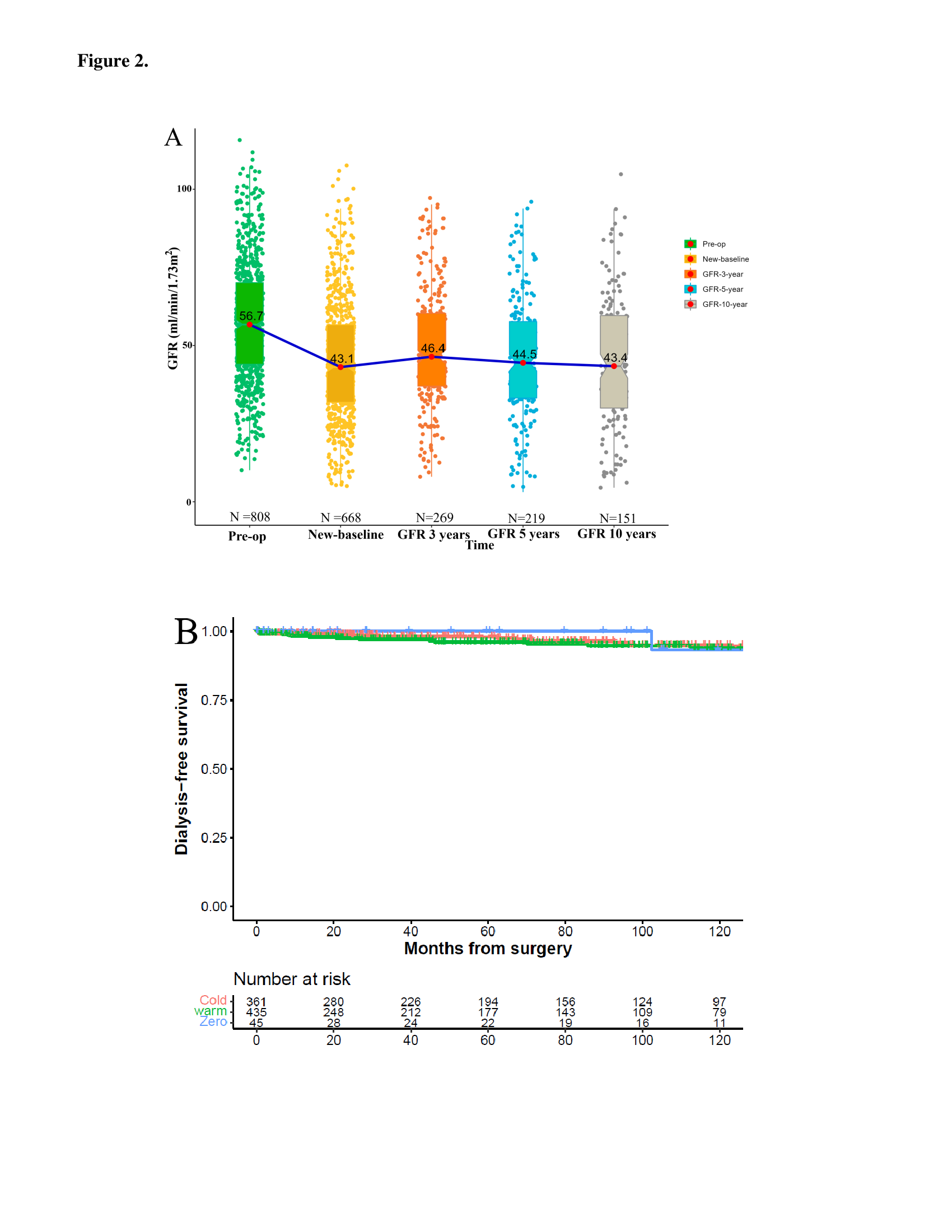
Introduction: Partial nephrectomy (PN) is the reference standard for management of renal mass in a solitary kidney (RMSK), although factors determining functional recovery in this setting remain ill-defined. Methods: 841 RMSK patients (1975-2022) managed with PN with functional data were identified, including 361/435/45 with cold/warm/zero ischemia, respectively. 155 patients also had necessary studies for detailed analysis of parenchymal volume preserved. Acute kidney injury (AKI) was classified by RIFLE (Risk/Injury/Failure/Loss/Endstage). Recovery from ischemia (Rec-Ischemia) was defined as glomerular filtration rate (GFR) saved normalized by parenchymal volume saved. Multivariable analysis was utilized to identify predictive factors for AKI and Rec-Ischemia. Results: Overall, median preoperative GFR was 56.7ml/min/1.73m2 and median new baseline and 5-year GFRs were 43.1 and 44.5 ml/min/1.73m2, respectively. Median follow-up was 55 months; 5-year dialysis-free survival was 97%. In the detailed analysis cohort, median warm (n=70)/cold(n=85) ischemia times were 25/34 minutes, respectively, and median preoperative, new baseline and 5-year GFRs were 57.8, 45.0 and 41.7 ml/min/1.73m2, respectively. Functional recovery correlated strongly with parenchymal volume preserved (r=0.84, p<0.001). Loss of parenchymal volume accounted for 69% of the total median GFR decline associated with PN, leaving only an average of 3-4 ml/min/1.73m2 due to ischemia and other factors. AKI occurred in 52% of patients and was Grade 2/3 in 20%. The only independent predictor of AKI was ischemia time, and independent predictors of Rec-Ischemia were age, warm ischemia, and AKI grade. Conclusions: The main determinant of functional recovery after PN in RMSK is parenchymal volume preservation. Type and duration of ischemia, AKI, and age also correlated, although altogether their contributions were less impactful. Our findings suggest multiple opportunities for optimizing functional outcomes although preservation of vascularized parenchymal volume remains predominant. Long-term function generally remains stable with dialysis only occasionally required. SOURCE OF Funding: none