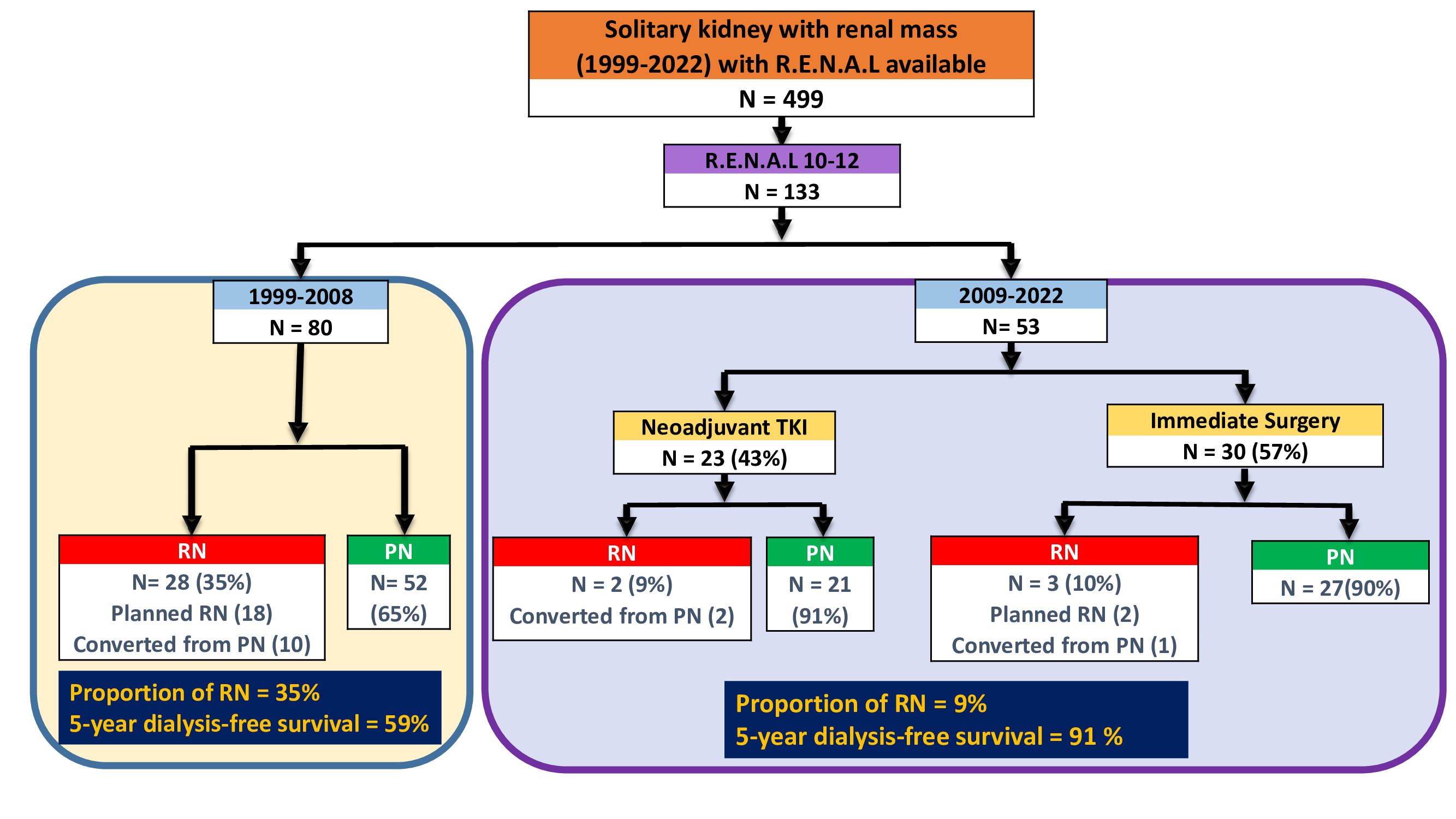
Introduction: Partial nephrectomy (PN) is preferred for renal mass in solitary kidney (RMSK), although tumors with high complexity (R.E.N.A.L=10-12) can be very challenging. Our objective was to evaluate the evolution of management for such patients, with focus on the pre-TKI (1999-2008) vs TKI (2009-2022) eras. Methods: 499 RMSK were managed from 1999-2022 at our center; 133 had high R.E.N.A.L., including 80/53 patients in the early/late timeframes, respectively. After 2009, 23 patients received tyrosine kinase inhibitor (TKI) before surgery, and 30 had immediate surgery. Achievement of PN was the primary outcome; other outcomes included adverse events and surgical complications related to TKI, and recurrence-free and overall survival (RFS/OS). Results: Overall, median R.E.N.A.L. and tumor diameter were 10/5.2 cm, respectively. Demographics, tumor diameter, and R.E.N.A.L were all similar in the early vs late cohorts. Non-confined pathology was found in 51%/58% of the early/late cohorts, respectively. In the late cohort, 23/53(43%) patients were selected for pre-surgical TKI. These 23 patients were the most challenging with increased median tumor diameter(7.1 vs. 4.4cm, p=0.02) and increased median R.E.N.A.L.(11 vs. 10, p=0.07). After TKI, median tumor diameter and R.E.N.A.L. were reduced to 5.6 cm and 9, and median tumor volume was reduced 59%. PN was accomplished in 21/23 (91%) of this cohort, and PN was also accomplished in 27/30 (90%) of the immediate surgery cases. In contrast, PN was only accomplished in 52/80(65%) patients in the pre-TKI era. 5-year dialysis-free survival was 91% vs 59% in the late vs early cohorts, respectively. Grade 3 adverse events related to TKI were observed in 11 patients (49%), and in this cohort, 5 urine leaks and one post-op. bleed were all managed successfully with conservative measures. Median follow-up was 41months; 5-year OS was 66%/71% in the early/late cohorts, respectively (p=0.5), while 5-year RFS were 73%/56%, respectively (p=0.07). Most recurrences were metastatic reflecting aggressive tumor biology, rather than failure of local management. Conclusions: RMSK with high tumor complexity is often locally advanced and challenging. Selective use of TKI may reduce the need for RN and augment dialysis-free survival. RFS mostly reflected aggressive tumor biology rather than failure of local management. SOURCE OF Funding: None