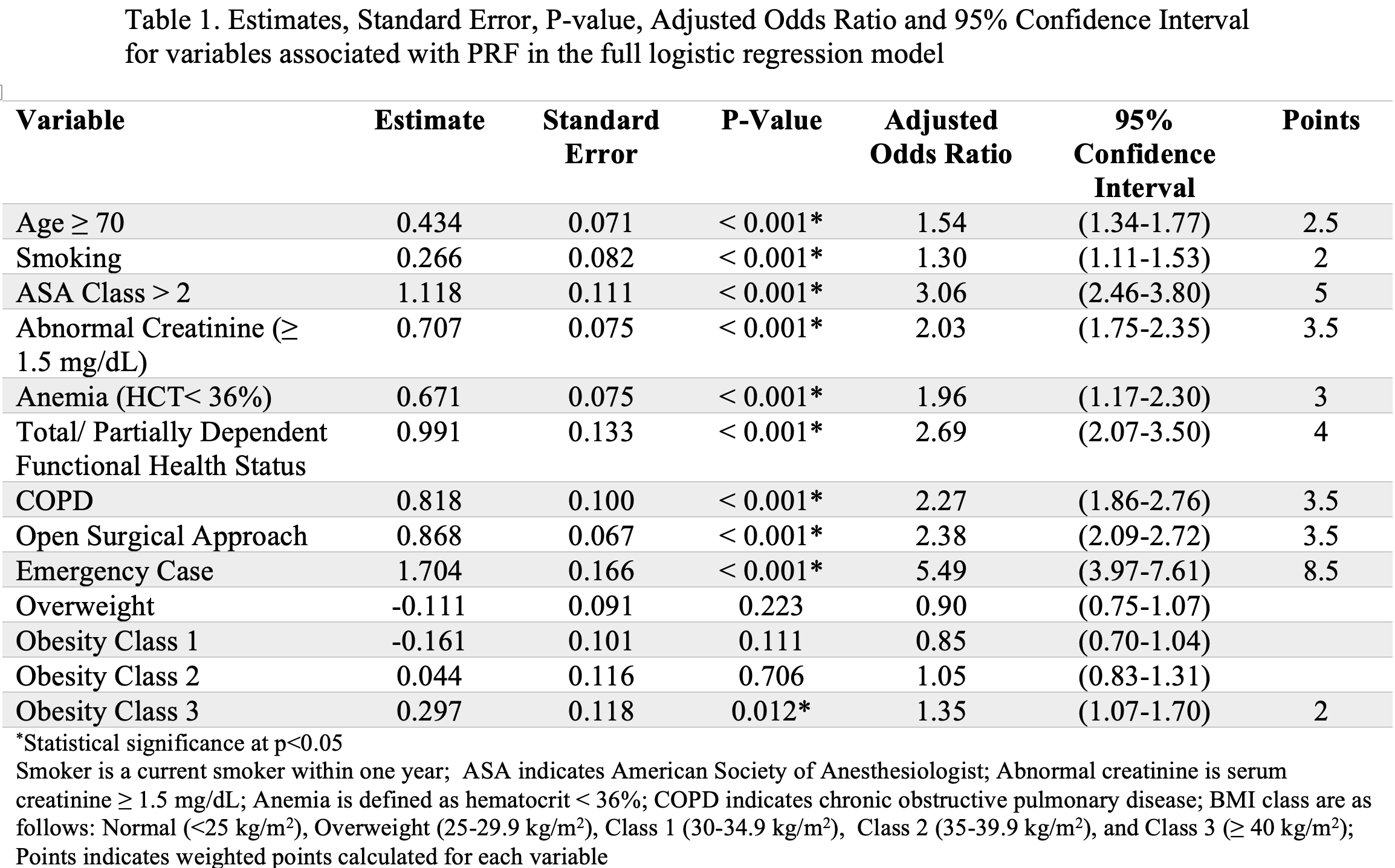
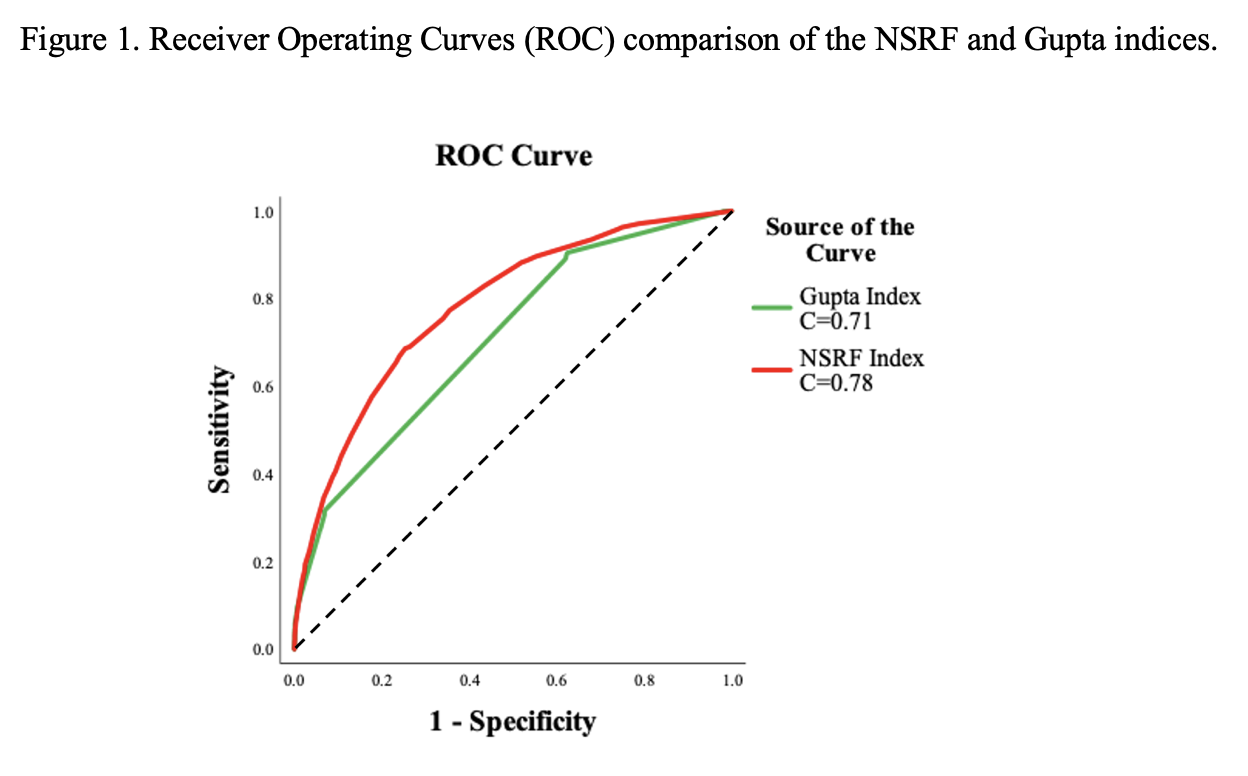
Introduction: Nephrectomy, either partial, simple, or radical, is the treatment of various renal pathologies that entails significant morbidity and mortality. Post-operative pulmonary failure is a major complication of nephrectomy that may lead to severe morbidity and mortality. We aimed to derive a nephrectomy specific post-operative respiratory failure index. Methods: We used the American College of Surgeons – National Surgical Quality Improvement Program database to select patients who underwent nephrectomy between the years 2005 and 2019. The outcome of interest was post-operative respiratory failure (PRF) defined as any incidence of unplanned intubation intraoperatively or postoperatively or requiring mechanical ventilation 48-hours after surgery. A multivariable logistic regression model was constructed, and model calibration and performance were assessed using a ROC analysis and the Hosmer-Lemeshow test. Finally, we derived the Nephrectomy Specific Respiratory Failure (NSRF) Index and compared it to Gupta’s index. Results: Our cohort included 79,526 patients that underwent nephrectomy of which 965 patients developed PRF. The final NSRF model encompassed ten variables: age, smoking status, American society of anesthesiology class, abnormal creatinine (= 1.5 mg/dL), anemia ( < 36%), functional health status, chronic obstructive pulmonary disease, surgical approach, emergency case, and obesity (= 40 kg/m2). The NSRF ROC analysis provided C-statistic = 0.78, calibration R2= 0.99 and proper goodness of fit. In comparison, the C-statistics of Gupta’s index was found to be 0.71 (p-value <0.001). Conclusions: The NSRF is a procedure tailored index for predicting post-operative respiratory failure. This index can be used in the pre-operative setting to help identify high risk patients who will require additional respiratory evaluation and preparation for their surgery. SOURCE OF Funding: None