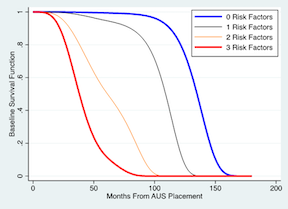
Introduction: Time to artificial urinary sphincter (AUS) removal or replacement is variable with no current means of forecasting individualized AUS survival times. We developed a prediction instrument for individualized counseling and follow-up planning. Methods: Post-prostatectomy patients with no history of urethral surgery, undergoing first-time AUS placement from 2000 to 2021, were identified as a training set for model specification. Erosion and infection related etiologies for removal were excluded. AUS survival, defined as time to replacement, was tested against clinical, urodynamic and surgical attributes. Variables were considered for Cox proportional hazard modeling based on theoretical associations with increased device use and exposure to pressure fluctuations in situ. The forward stepwise likelihood ratio process was used for variable selection. Discrimination was assessed with Harrell’s C-index. Excluded records served as a pseudo-validation cohort. Results: 341 records with urodynamic data were identified. A training cohort of 97 was derived with complete data and median follow up of 4.2 years (1.7, 8.3). There were 20 AUS replacements (20.6%) after a mean of 5.9 +/- 2.5 years for atrophy (55.0%) and mechanical failure (45.0%). A model was specified on five predictors: bladder neck contracture (HR=10.9, p<0.01), detrusor overactivity (HR=7.3, p<0.01), 24-hour pad weight (HR=0.99, p=0.09), bladder volume at strong sensation to void (HR=0.99 p=0.04) and baseline abdominal pressure (HR=0.92, p=0.07). The c-index was 0.82 for the training cohort and 0.92 when applied to the pseudo-validation cohort of 38 records with 5 (13.2%) AUS revisions. The baseline survival function without risk factors is compared in Figure 1 to that with detrusor overactivity, bladder neck contracture, and lower quartile of continuous predictors in additive fashion. Conclusions: Bladder mechanics and more frequent device use appear to be robust predictors of long-term AUS survival. A five-item prediction model demonstrated good discriminative capacity. The combination of urodynamic and voiding diary data can help augment follow-up planning and individualized counseling. SOURCE OF Funding: Boston Scientific Fellowship Grant

 photo")