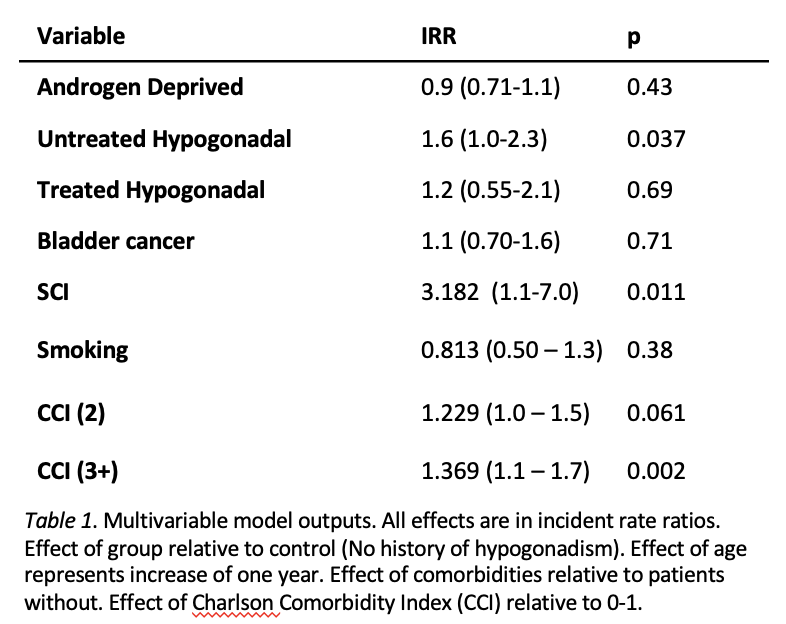
Introduction: The artificial urinary sphincter (AUS) has been the gold standard management in male stress urinary incontinence for the last 50 years. The most common complications requiring re-intervention include infection and erosion. Risk of late revision surgery or device removal range from 20-50%. Hypogonadism has been shown to impair wound healing and has been hypothesized to impact AUS device survival. Thus we sought to assess the incidence of AUS revision or removal in the setting of hypogonadism. Methods: Using IBM MarketScan, a commercial claims database, patients undergoing AUS were identified using Current Procedural Terminology (CPT) and ICD-10 procedure codes between 2008 and 2017. ICD-9/10 codes were used to identify patients with pre-operative diagnoses of hypogonadism. National drug codes (NDCs) and J-Codes were used to identify patients undergoing androgen deprivation therapy (ADT) or testosterone replacement therapy (TRT). Incident rate ratios (IRR) were assessed using a multivariate model to determine association of hypogonadism with AUS revision and/or explantation. Results: A total of 2740 men were identified that underwent primary AUS implantation of which 2228 had no prior history of hypogonadism or ADT therapy and were considered eugonadal. 512 (18.7%) men were hypogonadal or receiving TRT including active ADT 369 (13.5%) men, 92 (3.4%) hypogonadal without TRT, and 51 (1.9%) active TRT. On multivariate analysis, untreated hypogonadism (IRR 1.56; 95% CI [1.0-2.3]) was associated with an increased likelihood of re-operation when controlling for covariates. Active ADT (IRR 0.91; 95% CI [0.72-1.14]) and hypogonadism with active TRT (IRR 1.147; 95% CI [0.55-2.10] were not associated with increased risk of reoperation. Conclusions: In a cohort of 2740 patients undergoing primary AUS placement, untreated hypogonadism was associated with an increased likelihood of re-operation. TRT and ADT at the time of AUS surgery were not associated with increased rates of reoperation. SOURCE OF Funding: None