Session: MP80: Prostate Cancer: Localized: Surgical Therapy IV
MP80-01: The Surgical Learning Curve for Positive Surgical Margins after Robot-Assisted Radical Prostatectomy: Results from a Multi-Institutional Collaboration
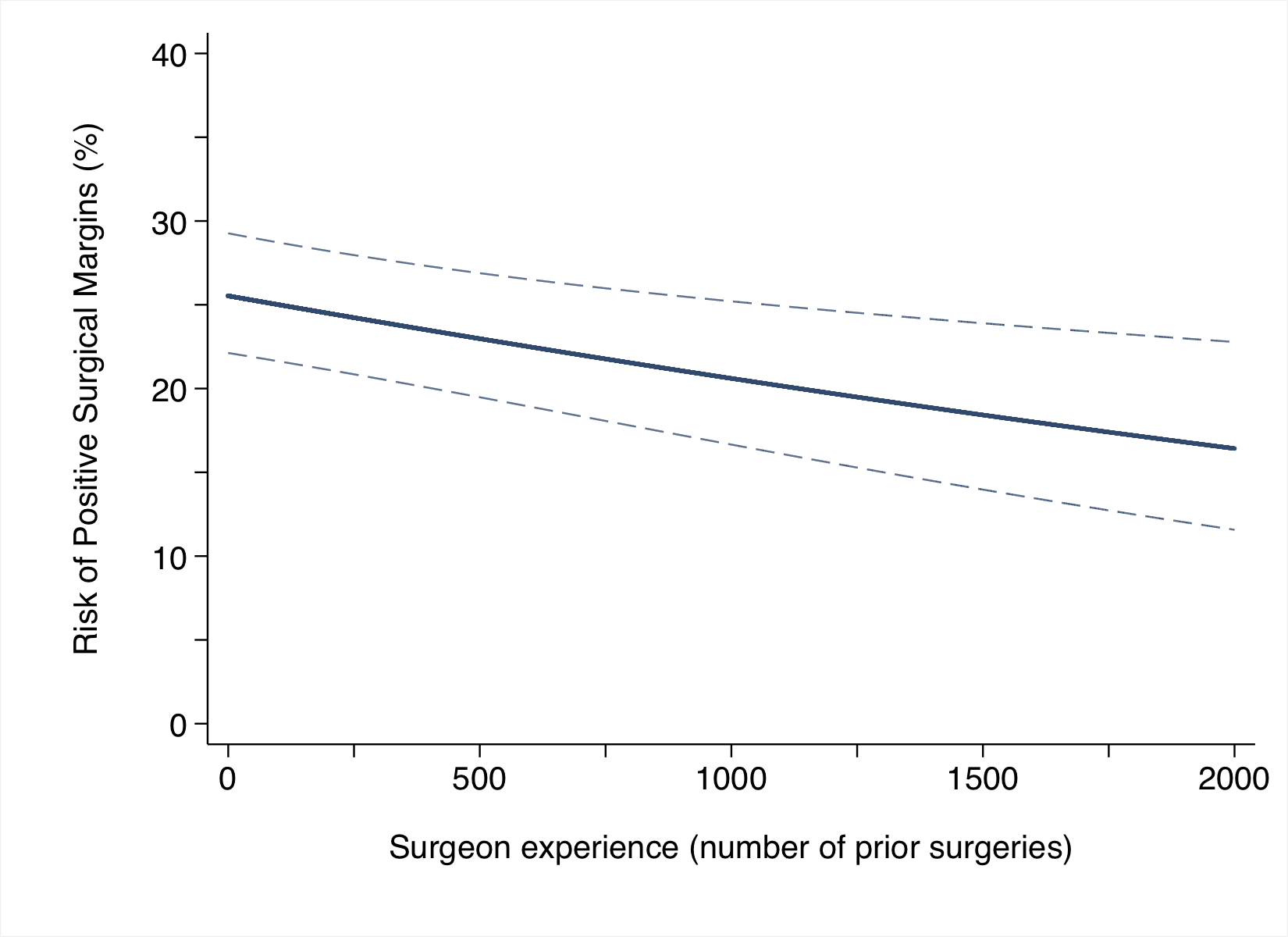
Introduction: In our preliminary single center experience, we described a learning curve for positive surgical margins (PSM) after robot-assisted radical prostatectomy (RARP). Now, we aim to characterize the learning curve for PSM after RARP in a multi-institutional collaboration. Methods: We analyzed data of 15,167 patients with prostate cancer treated with RARP by one of 83 surgeons at 14 institutions between 2003 and 2022. Multivariable models assessed the association between surgeon experience (number of RARPs done by the surgeon before the index patient’s operation) and PSM after surgery, with adjustment for preoperative PSA level, grade, stage, and year of surgery. Results: Median (interquartile range) PSA at surgery was 6.7 (5.0, 9.9) ng/ml. A total of 4,937 (33%), 2,404 (16%) and 938 (6%) patients had extra-capsular extension, International Society of Urologic Pathology group =4, and lymph node involvement on final pathology, respectively. Overall, 3,736 (25%) men had PSM at final pathology. After adjusting for case mix, we found a significant association between surgical experience and probability of PSM after surgery, with lower risk of PSM for greater surgeon experience (p=0.002; Figure 1). The probability of PSM for a patient treated by a surgeon with 10, 1000 and 2000 prior robotic procedures was 25.9% (95% confidence interval [CI]: 25.2%, 27.4%), 21.7% (95%CI: 20.6%, 22.3%) and 18% (95%CI: 16.1%, 18.6%), respectively (absolute risk difference between 10 and 2000 procedures: 7.86%; 95%CI: 6.9%, 10.7%). Results were unaltered after excluding surgeons with less than 100 prior RARPs performed at index patient’s operation (p=0.004), and repeating the analyses only including patients operated by surgeons who had performed fewer than 500 RARPs (p=0.023). Conclusions: In the largest series of patients exploring the association between surgical experience and risk of PSM after RARP, we confirmed our prior finding of a learning curve for PSM after RARP, with increasing prior experience associated with lower rate of PSM. Future investigations should now focus on what exactly more experienced surgeons do to avoid positive margins as compared to surgeons at an earlier stage of their career. SOURCE OF Funding: None