Session: MP80: Prostate Cancer: Localized: Surgical Therapy IV
MP80-06: Trends and Safety Profile of Same-Day Discharge for Robot-Assisted Laparoscopic Prostatectomy: A Retrospective Analysis of Two Tertiary Centers in the Northeastern United States
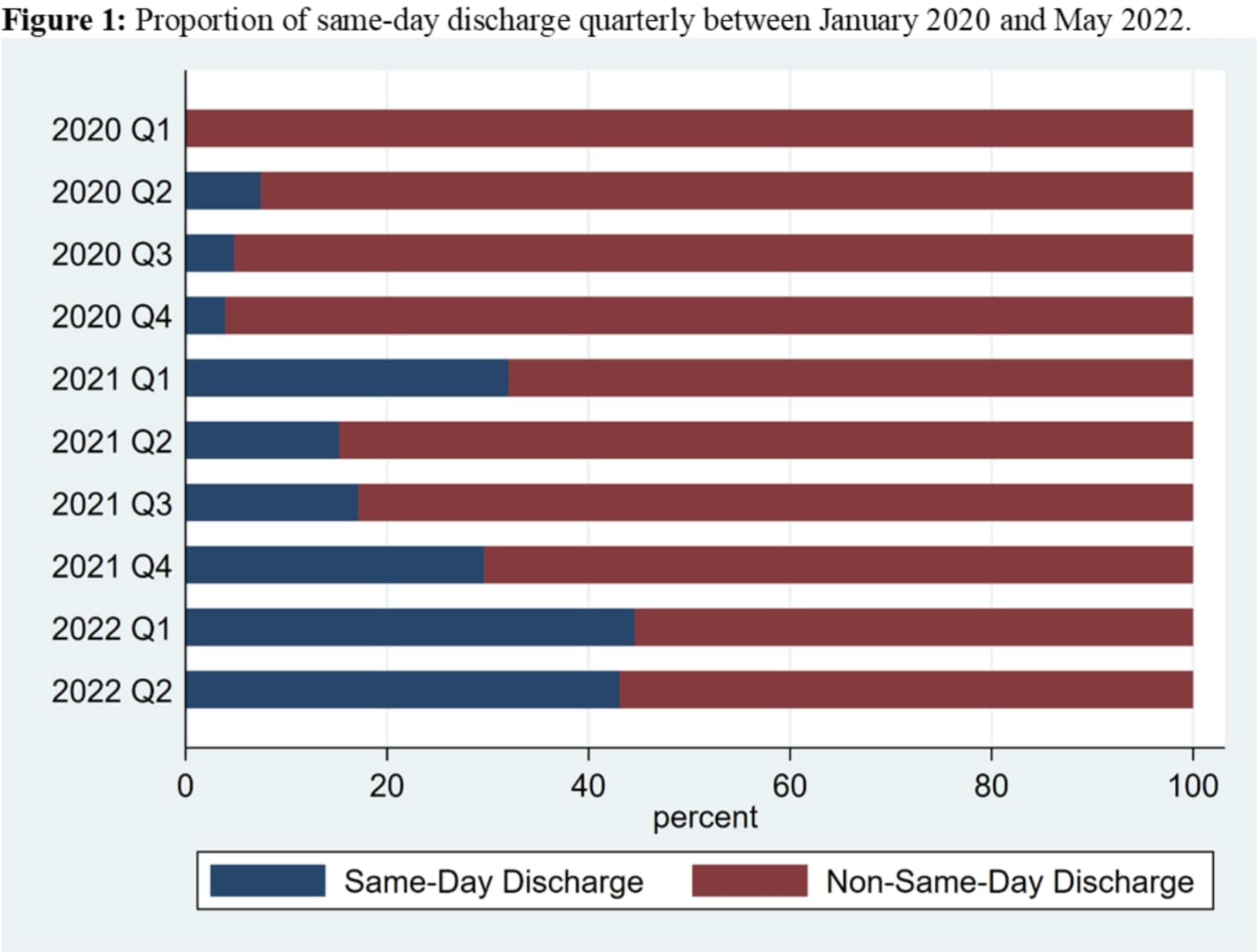
Introduction: We sought to (1) describe the predictors and trends of same-day discharge (SDD) and (2) compare the complications and readmissions among men who had SDD guided by the enhanced recovery after surgery pathway for RALP in two large tertiary care hospitals in the Northeastern United States. Methods: We retrospectively reviewed charts of men with prostate cancer who underwent RALP at our two institutions across 10 quarters between January 2020 and May 2022. We defined SDD as men who were discharged on the same day of surgery. Patient demographics, disease risk group, and social determinants of health were compared for SDD and non-SDD using Man-Whitney U test for continuous variables and chi-square or Fisher exact tests for categorical variables. Then, inverse probability of treatment weighting (IPTW) was used to balance patients covariates, facility site, and surgeon volume quartiles between SDD and non-SDD. An IPTW-adjusted logistic regression was fitted to examine the effect of SDD on 30-day postoperative complications and readmissions. Then, a logistic regression was fitted to identify the predictors of SDD. Results: Overall, 1,153 patients underwent RALP performed by ten surgeons, of which 224 (19.4%) had SDD. The proportion of SDD increased from 4.4% by the end of the fourth quarter in 2020 to 45% in the second quarter of 2022 (p < 0.01) (Figure 1). After weighting, there was no difference in baseline patient characteristics between SDD and non-SDD groups (standardized differences > 20%). SDD compared to non-SDD was neither associated with increased complications (OR=0.74; 95%CI [0.42-1.31]; p=0.30) nor increased readmissions (OR=0.99; 95%CI [0.44-2.22]; p=0.98). The only predictor of SDD were the facility where the surgery was performed and whether it was performed by a high-volume surgeon. Conclusions: In our health system, SDD is increasingly adopted by our surgeons. SDD is associated with similar perioperative outcomes compared to non-SDD. Future larger cohort analysis or clinical trials are needed to confirm our findings. SOURCE OF Funding: None

 photo")