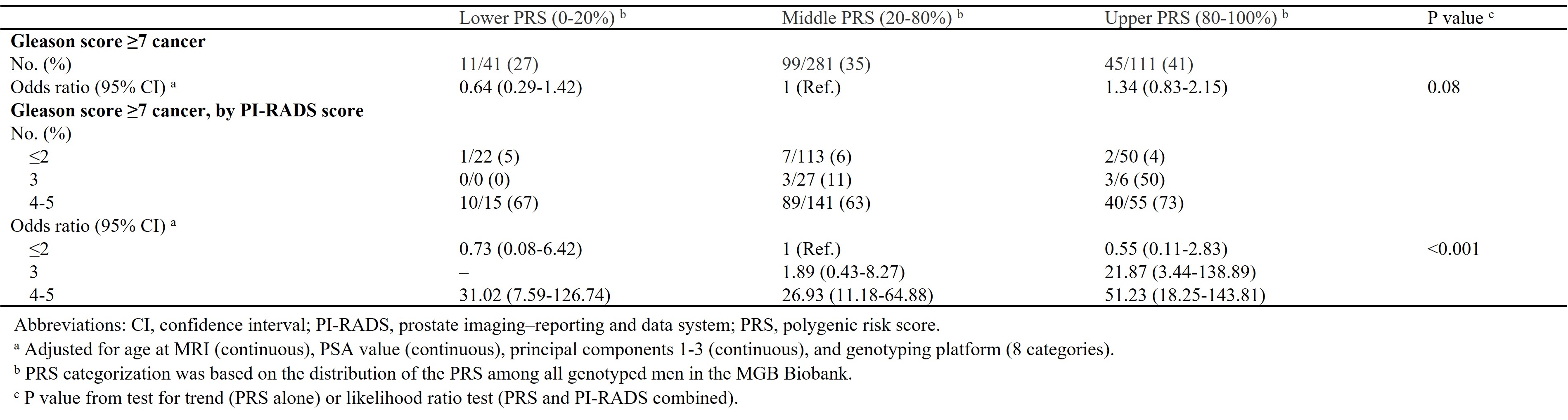
Introduction: Polygenetic risk scores (PRS) use a genetic fingerprint to identify men at risk of prostate cancer (PCa). Unfortunately, PRS cannot discriminate indolent from aggressive disease. Multiparametric MRI (mpMRI) is an excellent tool to identify Gleason score (GS) =7 disease. We postulated that combining PRS with mpMRI would improve ability to identify clinically significant PCa. This study aims to investigate the predictive capacity of combination of PRS and MRI in identifying clinically relevant PCa. Methods: We identified men in the Mass General Brigham Biobank who underwent genotyping and prostate mpMRI from 2015-2019. Inclusion criteria consisted of =1 prostate MRI performed within 1 year of diagnosis and no treatment for PCa prior to MRI. For each PRS strata (lower: 0-20%, middle: 20-80%, upper: 80-100%), we examined frequency of clinically significant PCa (GS =7) by PI-RADS category (=2, 3, 4-5). Logistic regression adjusting for age at MRI, PSA, principal components 1-3, and genotyping platform was used to examine the association between PI-RADS category and clinically significant PCa across PRS categories. Results: We identified 433 men of European ancestry that were included and categorized based on quantiles of the PRS (lower, middle, upper) and PI-RADS score (=2, 3, 4-5). Men in the upper PRS category had highest frequency of clinically significant PCa (41%) compared to the middle (35%) and lower PRS (27%) category. Men in the upper PRS category had the highest detection rate of clinically significant PCa among men within PI-RADS score of 4-5 (73%) compared to the middle (63%) and the lower (67%) PRS category. The associate was strongest in patients with high PRS and PIRADs 4/5 who were ~50 times more likely to harbor GS =7 than men with average PRS and normal mpMRI. Measured by AUC, discriminatory ability of clinically significant cancer was 0.79 for PI-RADS, PSA value and age, and 0.81 for PI-RADS, PSA value, age and the PRS. Conclusions: Combination of PRS and mpMRI PI-RADS score has potential to improve risk stratification of men at risk for clinically significant PCa. Our results support a paradigm where only men with elevated PRS undergo screening, thereby identifying men at risk and sparing low risk men the side effects of biopsy and treatment. SOURCE OF Funding: DiNovi Family Foundation, William Casey, Prostate Cancer Foundation, Swedish Society for Medical Research, Swedish Cancer Society