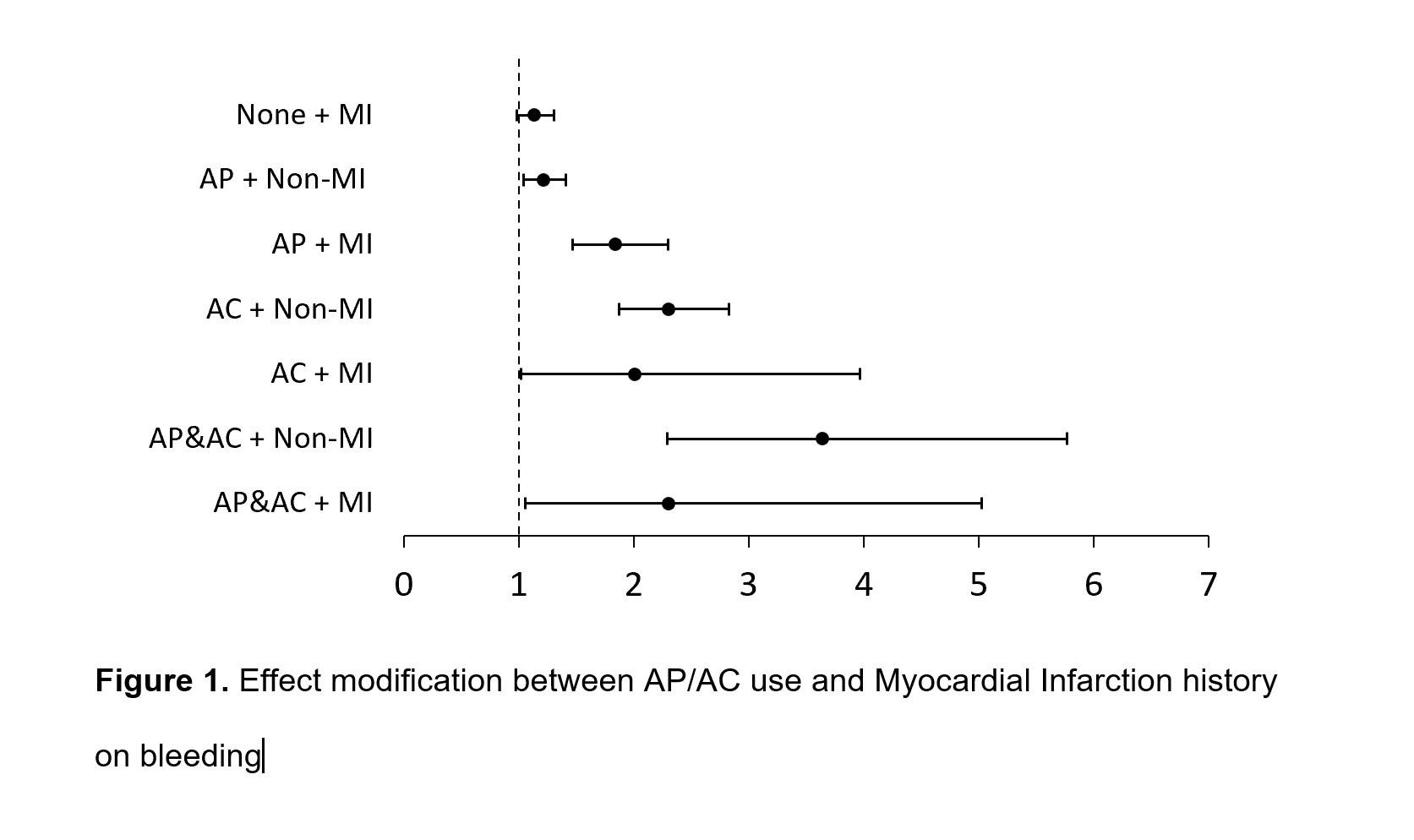
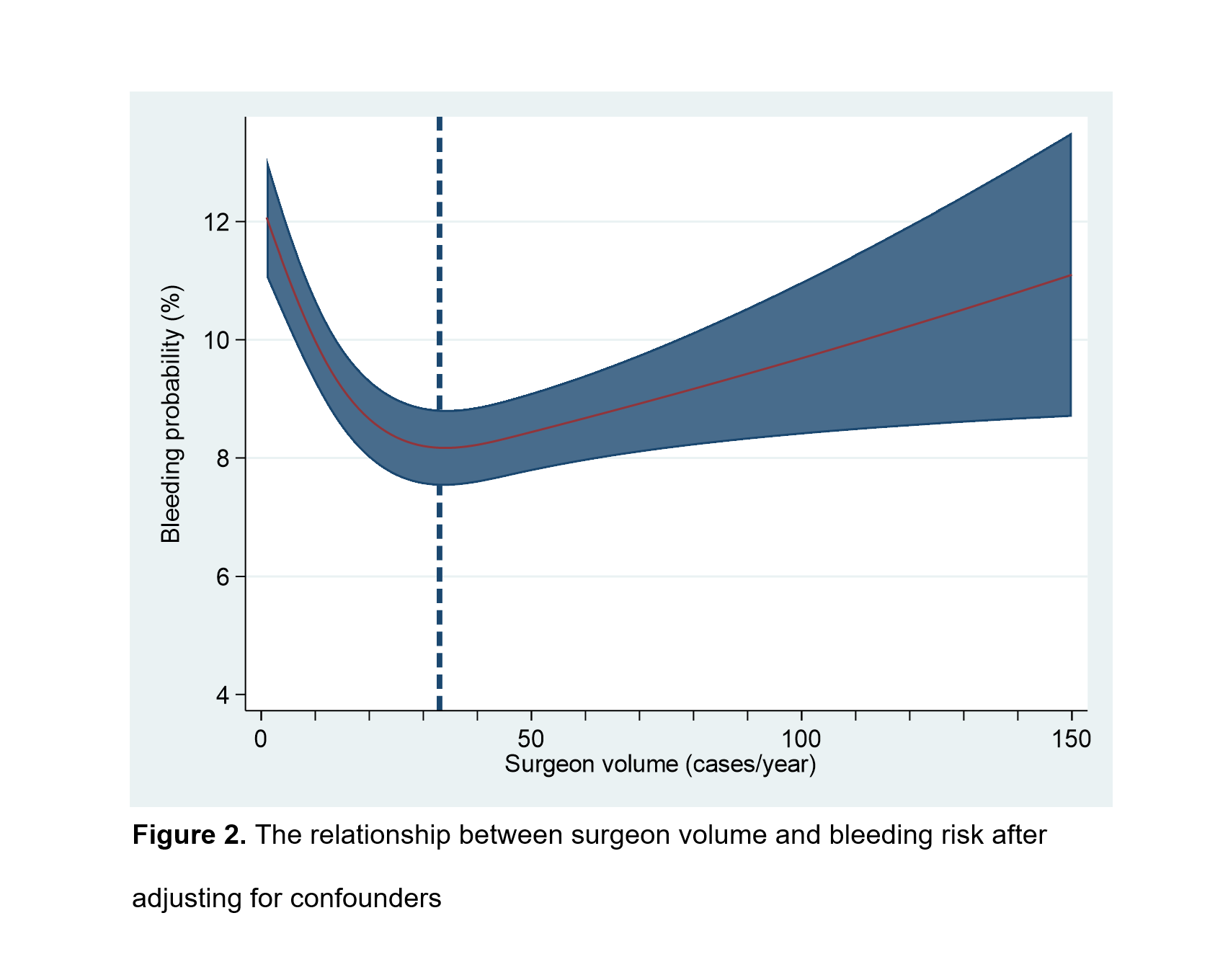
Introduction: Whether perioperative period oral antiplatelet (AP) and anticoagulant (AC) drugs use can lead to bleeding in PN is controversial. This study analyzes the association between oral AP/AC use and bleeding complications in partial nephrectomy in a large cohort. Methods: Using the Premier Hospital Database, we performed a retrospective cohort study of patients undergoing partial nephrectomy to manage kidney cancer and renal masses from 2003 to 2020. The study cohort was limited to adult patients undergoing elective surgery. Using administrative codes and billing, we assessed for an association between AP/AC drug use and bleeding complication using mixed-effects multiple logistic regression models controlling for a wide range of clinical-demographic, surgical, and hospital factors. The primary outcome was bleeding within 90 days in or after surgery. Secondary outcomes were mortality rate 90 days after surgery and length of hospital stay. Results: The study cohort comprised 48,112 partial nephrectomy patients, of which 10.9% had bleeding complications. Mixed-effects multivariable logistic regression models revealed that AP was associated with 31% increased odds for bleeding (OR 1.31; 95% CI: 1.15-1.49; p<0.01) and AC was associated with 2.25 times odds for bleeding compared with none users (OR 2.25; 95% CI: 1.85-2.74; p<0.01), AP and AC combination group was associated with the most bleeding risk (OR 3.09; 95% CI: 2.q4-4.74; p<0.01). An effect modification of oral AP drug use and Myocardial infarction (MI) history was detected, which is shown in Figure 1. The relationship between surgeon volume and bleeding risk was presented as a "J" shape (Figure 2). More than 33 cases/year for PN surgeons entered a plateau phase and slightly increased the bleeding risk. Conclusions: AC/AP use is associated with a significant increase in bleeding complications following partial nephrectomy surgery; Compared with AP, AC induces more probability of bleeding; AP and AC combination lead to even more bleeding risk. SOURCE OF Funding: None