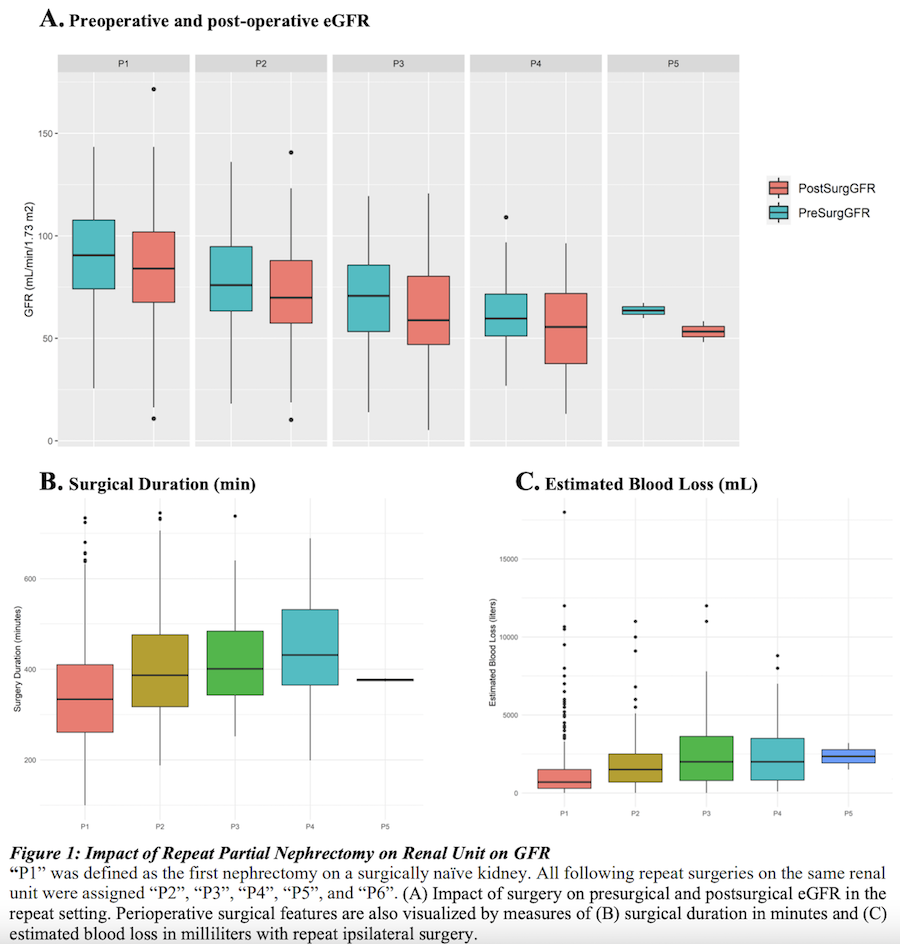
Introduction: Repeat partial nephrectomy (RePN) offers advantages for the treatment of recurrent, multifocal renal masses. RePN has been demonstrated to be technically feasibile and delays the onset of renal failure. However, there are inherent intraoperative complexity and post-operative challenges with RePN. We studied the largest known population of patients undergoing RePN in order to characterize intra- and post-operative complications as well as renal functional outcomes to fully appreciate risks of and benefit to this operative strategy. Methods: Retrospective query of an institutional registry of nephrectomies was conducted. Demographic data, serum creatinine (SCr) and protein dipstick results were assessed within one week prior to surgery, and postoperative function assessments were studied within a year of surgery. SCr was used to calculate eGFR using CKD-EPI 2021. RePN was defined as serial surgical resection of the ipsilateral renal unit. Statistical analysis was conducted on R Studio v 4.1.1. Results: A total of 1,131 PNs performed on 663 patients at a single center were retrospectively evaluated. In reoperative cases, median number of operations per renal unit was 2 (range: 2-6). There was a stepwise decline in eGFR with an average decline of 6.1 with each RePN (p < 0.001). With each subsequent nephrectomy, surgical duration (p < 0.001), and estimated blood loss (p < 0.001) increased. Patients encountered an increased incidence of anemia when controlling for gender, race, solitary kidney, and preoperative GFR (p=0.007). On multivariate analysis of post-surgical GFR, the number of tumors removed, largest tumor removed, age, total previous partial nephrectomies, presurgical GFR, pre-operative proteinuria and solitary kidney were significant independent predictors. Number of tumors removed, number of previous PN, and open surgical approach were significant predictors of surgical complications. Conclusions: Repeated PN contributes to renal functional decline, anemia, and an increased risk of surgical complications. Intraoperative blood loss and surgical duration increase with subsequent nephrectomy. These impacts must be fully appreciated to optimize patient counseling regarding surgical management and sequencing of available therapies. SOURCE OF Funding: NIH MRSP