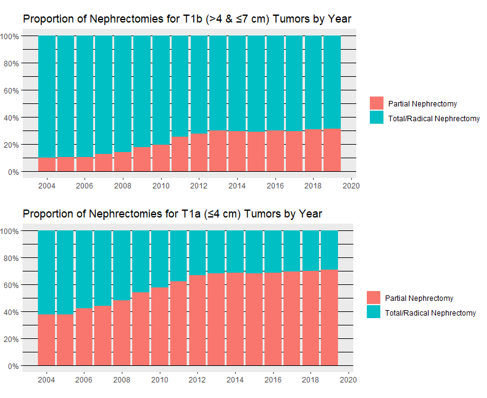
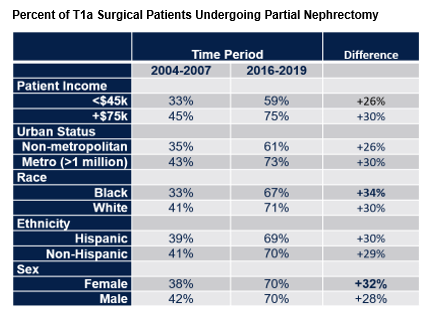
Introduction: Beginning in the late 1990s partial nephrectomy (PN) became increasingly common for treatment of renal cell carcinoma as an alternative to radical (or total) nephrectomy (RN). Early work established disparities within whom received partial nephrectomy with black, female, and low-income patients less likely to receive partial nephrectomy. Recent trends in the continued adoption and demographic disparities within PN are not known. Methods: Using 2004-2019 SEER data we identified 131,527 renal cell carcinoma patients with tumors between 1.0 and 10 cm who underwent nephrectomy, PN or RN. We assessed predictors of partial nephrectomy using multivariable logistic regression assessing tumor size, treatment year, income, metropolitan status, race, and ethnicity as independent predictors. We also report proportions of nephrectomies performed by PN within different groups across this period. Results: Between 2004 and 2019 the mean tumor size treated with PN increased from 3.0 cm (95% CI 2.9-3.1) to 3.3 cm (95% CI 3.2-3.3) and the percent of excised T1a tumors, =4 cm, treated with PN increased from 37.6% to 70.6% (Figures 1 & 2). While controlling for tumor size and treatment year on multivariable logistic regression, Black, Hispanic, non-metropolitan, and lower income patients were all less likely to receive partial nephrectomy (Odds ratios of 0.82, 0.84, 0.83, and 0.70, all p<0.001). The gap in percentage of patient receiving partial nephrectomy for T1a tumors appeared to be eliminated for female patients, narrow for black patients, but widen for poor and rural patients across the study period (Table 1). Conclusions: Partial nephrectomy for renal cell carcinoma has become increasingly common over the past 16 years with some plateau over the last 5 years. Despite this, demographic disparities in utilization of partial nephrectomy remain pronounced, particularly for low-income and rural patients. SOURCE OF Funding: none