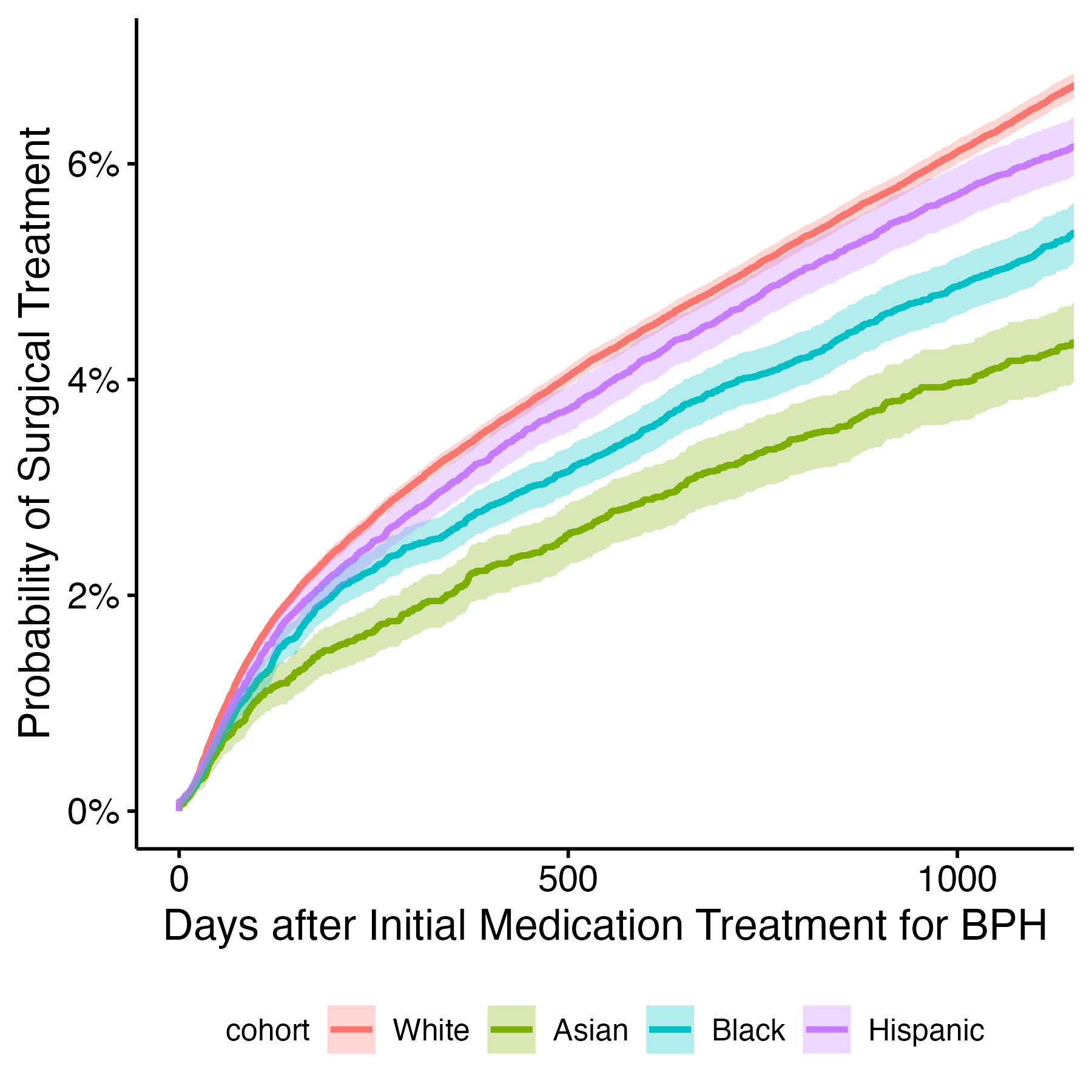
Introduction: Benign Prostatic Hyperplasia (BPH) is a common urological condition treated medically and/or surgically. Racial disparities persist throughout medicine in both access to care and treatment of disease. The objective of this study is to compare the rates of surgical treatment in BPH across racial and ethnic groups. Methods: A retrospective cohort study was performed using Komodo Health’s claims database of 330 million patients from 2017-2021. Deidentified male patients older than 40, continuously enrolled for 1 year prior/3 years after initial medication treatment of BPH, were abstracted and cleaned in a standardized pipeline. Patients were required to have at least 1 BPH diagnosis code and no history of malignancy. Diagnosis of BPH and medical/surgical treatment was determined by ICD, NDC, and CPT codes. Logistic regression was used to determine surgical rates between races by adjusting for age, charlson’s comorbidity index, and the use of BPH medications. The cumulative incidence of surgical treatment was summarized using one minus the Kaplan-Meier(KM) estimator. All analyses were conducted in R 4.2.1. Results: Of 330 million patients, 246,959 were included. This included 179,496 (72.7%) White, 11,812 (4.7%) Asian, 24,959 (10.1%) Black, and 30,692 (12.4%) Hispanic patients. 49.5% were over 65 and 6.2% had received surgery within 3 years of initiating medication. Black (5.1%) and Asian (4.2%) patients were less likely than White (6.5%) and Hispanic (6.0%) patients to have surgery in this time frame. The median time to surgery was 342 days. Variation was seen across races: White: 340 days, Asian: 368 days, Black: 343 days, and Hispanic: 345 days. In the logistic regression model adjusting for age, comorbidities, and medication use, White patients were more likely to receive surgery than Asian (OR 0.58, p<0.001), Black (OR 0.82, p<0.001), and Hispanic (OR 0.90, p<0.001) patients. The cumulative incidence curve (1- KM) is seen in Figure 1. Conclusions: Black, Asian, and Hispanic men were less likely than White men to receive surgical treatment after medication treatment of BPH. This could be attributed to barriers to access, trust in the medical system, or systematic bias. Further studies are needed to discern potential causes and meaningful solutions to ensure equitable access to care. SOURCE OF Funding: NA