MP56-09: Neoadjuvant Pembrolizumab Shows Promise as Effective Systemic Therapy Prior to Radical Cystectomy for Cisplatin-Ineligible Muscle Invasive Bladder Cancer
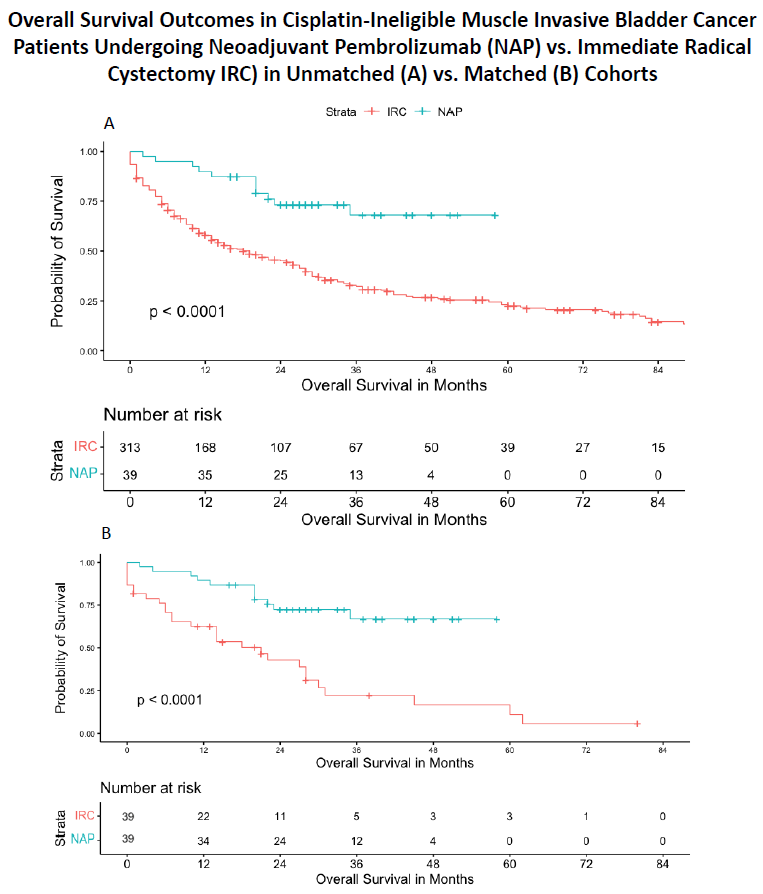
Introduction: There is an unmet clinical need for systemic treatment in patients with muscle-invasive bladder cancer (MIBC) who are ineligible for cisplatin-based neoadjuvant chemotherapy. We aimed to compare pathologic response and survival outcomes in cisplatin-ineligible patients receiving neoadjuvant pembrolizumab (NAP) vs. immediate radical cystectomy (IRC). Methods: Cisplatin-ineligible patients with cT2-4N0M0 MIBC were identified from the PURE-01 trial and compared against cisplatin-ineligible MIBC patients treated with immediate radical cystectomy (IRC). Overall survival (OS) analysis was performed using the Kaplan-Meier method and Log-Rank functions. Cox-proportional hazards modelling was used to determine variable contribution to survival. Propensity score matching was performed for IRC and NAP patients based on pre-cystectomy ECOG status, GFR, age, sex, and clinical T stage. An exploratory analysis also matched patients by pathologic T stage. Statistical analysis was performed using R. Results: Thirty-nine cisplatin-ineligible patients treated with NAP were identified from PURE-01, and compared against 313 cisplatin-ineligible patients undergoing IRC (Figure 1A). OS was prolonged in the NAP patients, with median survival of 19 months in the IRC vs. not reached (NR) in the NAP group (p < 0.01). Thirty-nine patients were identified from the IRC cohort after propensity matching, with comparable baseline clinicopathologic data. Patients receiving NAP experienced a higher complete response rate on final pathology (pT0: 33% vs. 13%, p=0.03). Median OS was prolonged in the NAP group (NR vs. 21.0mo, p<0.01), specifically at 12mo (89% vs. 57%), 24mo (64% vs. 28%), and 36 months after surgery (33% vs. 13% ) (p < 0.01). On Cox Proportional Hazards Modelling, patients undergoing IRC demonstrated worse OS with a hazard ratio of 2.0 (95% CI 1.1 - 3.89). Conclusions: Cisplatin-ineligible patients receiving NAP for muscle invasive bladder cancer had a higher rate of downstaging and a survival advantage over patients who underwent IRC. Results of ongoing prospective randomized trials will help validate these findings and provide therapeutic options to cisplatin-ineligible patients. SOURCE OF Funding: NA