Session: MP61: Prostate Cancer: Localized: Surgical Therapy II
MP61-12: Which Men With cN1 Prostate Cancer At PSMA PET/CT Represent The Ideal Candidate To Radical Prostatectomy? Development Of A Novel Risk Stratification Tool For Individualized Approaches Based On A Large, Multi-Institutional Series
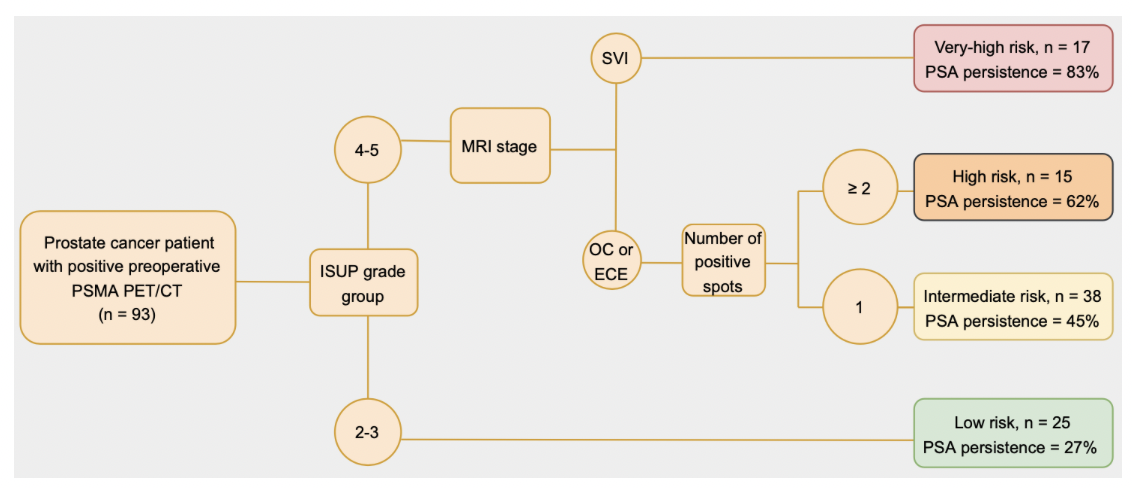
Introduction: Limited data is available to identify men who would benefit the most from radical prostatectomy (RP) in prostate cancer (PCa) patients with clinical lymphadenopathies (cN+) at PSMA PET and, on the other hand, to select patients for proper management. We aimed at assessing predictors of early recurrence in surgically managed PCa patients with cN+ at PSMA PET scan by integrating clinical, magnetic resonance imaging (MRI) and PET parameters. Methods: We identified 662 patients treated with RP and lymph node dissection who received preoperative PSMA PET between 2017 and 2022 at nine referral Centers. We selected 93 patients with positive nodal uptake at preoperative PSMA PET. The study outcome was PSA persistence, defined as a PSA =0.1ng/ml at first postoperative measurement. Multivariable logistic regression tested predictors of persistence. Covariates consisted of biopsy ISUP grade group (IGG) (2-3 vs 4-5), stage at MRI (organ-confined disease [OC] vs. extracapsular extension [ECE] vs. seminal vesicles invasion [SVI)) and number of positive spots at PET scan. Regression tree analysis stratified patients into risk groups based on their preoperative characteristics. Results: Median number of positive spots at preoperative PET was 2. LNI was detected in 64 patients (69%). Comparing PSMA PET and final pathology, concordance of positive nodes location was 85%. 32 patients (34%) experienced PSA persistence after RP. At multivariable analyses, biopsy IGG 4-5 represented the strongest predictor of PSA persistence (OR: 2.44; p=0.001). At regression tree analysis, patients were stratified in four risk group according to IGG, number of positive spots at PET and stage at MRI (Fig.1). This model depicted a good discrimination (AUC 78%). Notably, patients in high and very-high risk groups showed higher PSA persistence (62 and 83%, respectively) compared to low-risk group (27%). Conclusions: Patients with IGG 2-3, as well as patients with IGG 4-5 but with OC or ECE at MRI and a single positive spot at PET are those where RP may achieve the best oncological. Conversely, patients with high GG and SVI or >1 spots at PSMA PET should be considered as potentially affected by a systemic disease upfront. SOURCE OF Funding: none