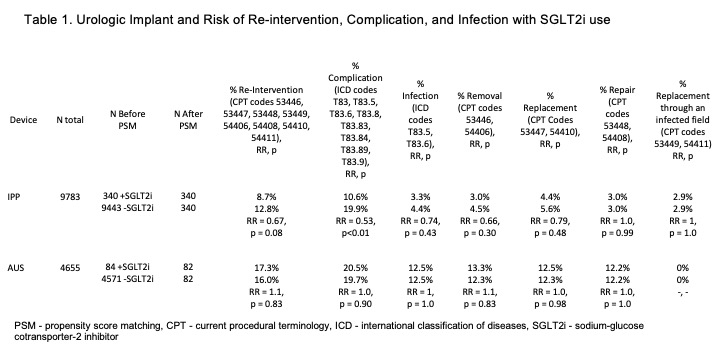
Introduction: Sodium-glucose co-transporter 2 inhibitors (SGLT2i) prevent the reabsorption of glucose and facilitate its excretion in urine. Patients taking these medications are at a hypothetical increased risk of urinary tract and genital infections given the mechanism of action. We questioned whether patients taking SGLT2i would be at an increased risk of genitourinary device infection or failure. Methods: We queried the TriNetX database for all adult male patients undergoing Artificial Urinary Sphincter (AUS) or Inflatable Penile Prosthesis (IPP). For each implant, we separated patients into cohorts defined by those taking an SGLT2i within 1 year before and/or after surgery and those not taking an SGLT2i. Cohorts and outcomes were defined using Current Procedural Terminology (CPT) and International Classification of Diseases (ICD-10) codes. We used Age, Race, Ethnicity, Body Mass Index (BMI), Diabetes, smoking history, history of radiation, and history of prostatectomy to generate propensity score matching (PSM). Our primary outcome was need for re-intervention (revision, removal, or replacement surgery) at any point after implantation based on CPT codes. Secondary outcomes included infection rate and overall complication rate based on ICD-10 codes. Analytics were performed via TriNetX which calculated Risk Ratios. Results: Analyses were run on October 14th, 2022. There were 9783 patients who underwent IPP and 4655 who underwent AUS (Table 1). After PSM, there were 340 and 82 patients in each IPP and AUS cohort with similar ages (60.9 vs 60.7 years; 68.6 vs 68.7 years) and similar comorbidity profiles except patients with an IPP on an SGLT2i had higher average BMI (31.9 vs 30.6 kg/m2, p=0.01). The average Hemoglobin A1c level was higher for patients taking an SGLT2i; 8.0% vs 7.1% (p < 0.01) for IPP and 7.9% vs 6.9% (p=0.01) for AUS. Patients with an IPP on an SGLT2i were at a lower risk of overall complication (10.6% vs 19.9%, RR 0.53, p<0.01). There was no difference for AUS and risk of complication and no difference for either implant on risk of infection or re-intervention. Conclusions: Patients taking SGLT2is may be safely offered urologic implants. Patients taking an SGLT2 had a lower risk of complication for IPP, and there were similar rates of infection and re-intervention for both IPP and AUS. SOURCE OF Funding: none