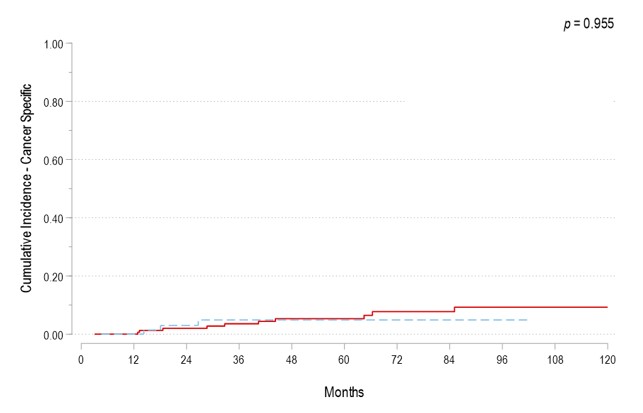
Introduction: European Association of Urology (EAU) guidelines recommend offering immediate radical cystectomy (iRC) to all very high-risk (VHR) non-muscle invasive bladder cancer (NMIBC) patients and reserving BCG for only those who refuse or are unfit for RC. Herein, we assessed survival outcomes of VHR NMIBC patients treated with BCG versus iRC. Methods: We performed an IRB approved retrospective study analyzing VHR NMIBC patients according to the EAU definition diagnosed between 2000 and 2020. Survival outcomes between the following patient cohorts were compared: 1) Immediate RC versus BCG and 2) Immediate RC versus delayed RC. Primary endpoint was overall-(OS) and cancer-specific survival (CSS). The cumulative incidence (CI) method was used to estimate the risk of cancer-specific mortality (CSM) after accounting for other causes of death as a competing risk event. Multivariate competing-risks regression analyses were used to predict CSM. Results: A total of 235 VHR patients were identified (157 BCG versus 78 iRC). The median follow-up was 45.8 months. Patients treated with iRC were younger (68 yrs vs. 72 yrs; p<0.01), had a higher prevalence of lymphovascular invasion (LVI) (29.5% vs 4.5%; p<0.01) and variant histology (53.8% vs 16.6%; p<0.01) at diagnosis. The 5-yr OS and CSM were 80.2% and 5.3% in patients undergoing BCG and 88.1% and 4.9% in patients undergoing iRC. Survival outcomes did not significantly differ between the two groups (p=0.604 and p=0.955, respectively; Figure). Treatment strategy was not associated with CSM in the multivariate competing-risk regression model (Sub-standardized Hazard ratio (SHR): 1.54; 95%CI 0.24 – 9.68; p=0.65). Among the patients treated with BCG, 5-yr PF rate was 82.6%. A total of 39 (24.8%) patients underwent delayed RC following recurrence after BCG. Patients who underwent delayed RC did not exhibit worse oncological outcomes relative to those treated with iRC (SHR: 0.66, 95% CI: 0.17-2.61, p=0.56). Conclusions: Survival outcomes following initial treatment with intravesical BCG (with delayed RC if needed) for selected VHR NMIBC can be effective and oncologically safe. SOURCE OF Funding: This research was supported by the Wayne B. Duddlesten Professorship in Cancer Research, the Raymond and Maria Floyd Bladder Cancer Research Foundation Grant, NIH/NCI UTMD Anderson SPORE in Genitourinary Cancer (P50CA091846), the Cancer Center Support Grant (NCI Grant P30 CA016672)