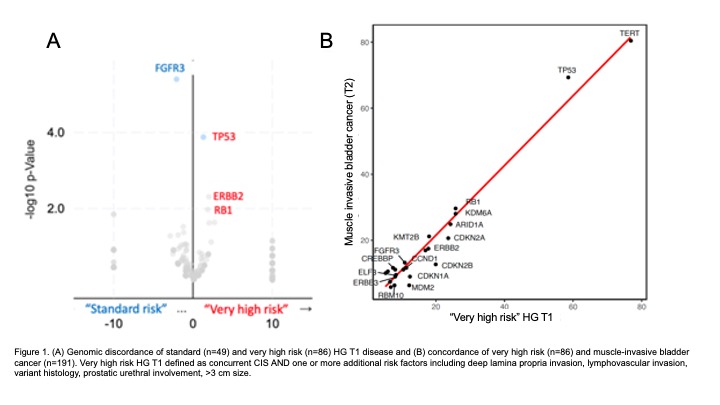
Introduction: High grade non-muscle invasive bladder cancer invading the lamina propria (HG T1) exhibits variable clinical behavior. Existing risk stratification approaches by clinicopathologic alone are limited in determining who will benefit most from immediate radical cystectomy (RC) versus BCG. We report contemporary outcomes of patients managed with BCG or immediate RC and comparative mutational landscape across the spectrum of HG T1 disease. Methods: This was a single-center retrospective cohort study of patients newly diagnosed with HG T1 non-muscle invasive bladder cancer between 2014 and 2020 >18 months of follow up. All included patients underwent restaging TURBT with confirmed T1 by TURBT/EUA/imaging. Targeted exome sequencing with MSK-IMPACT was performed on 139 HG T1 tumors and 191 T2 tumors. Results: 390 patients were included with median follow up time of 35 months (IQR 19-59 months). 308 were managed with intravesical BCG and 82 immediate RC. Patients selected for immediate RC were younger (median age 66 vs 69, p<0.001) and had higher rates of concurrent CIS (78 vs 53%, p<0.001), deep lamina propria invasion (37 vs 17%, p<0.001), lymphovascular invasion (7 vs 0.3%, p<0.001), and larger tumor size (4.3 cm vs 3.3 cm, p=0.007). Of the 82 patients who immediate radical cystectomy (BCG naïve), 32 (40%) were upstaged to pT2 and/or N+ disease at RC. Persistent pT1 disease at re-resection and the presence of variant histology were associated with pathologic upstaging (p < 0.01), while tumor size, concurrent CIS, bladder neck involvement, or prostatic urethra involvement were not. Compared to patients without additional risk factors, patients with CIS and at least one additional risk (e.g . “very high risk” T1 disease) harbored more TP53, ERBB2/Her2, and RB1 mutations and fewer FGFR3 mutations and a genomic profile more similar to T2 tumors than NMIBC (Figure 1). Conclusions: Very high risk T1 tumors are genomically similar to muscle-invasive tumors and are enriched in targetable alterations including ERBB2/Her2. Integration of genomic sequencing with clinical and pathologic features of HG T1 disease may improve risk stratification and treatment selection. SOURCE OF Funding: Ruth L. Kirschstein National Research Service Award T32CA082088 American Society of Clinical Oncology Young Investigator Award (YIA) Award