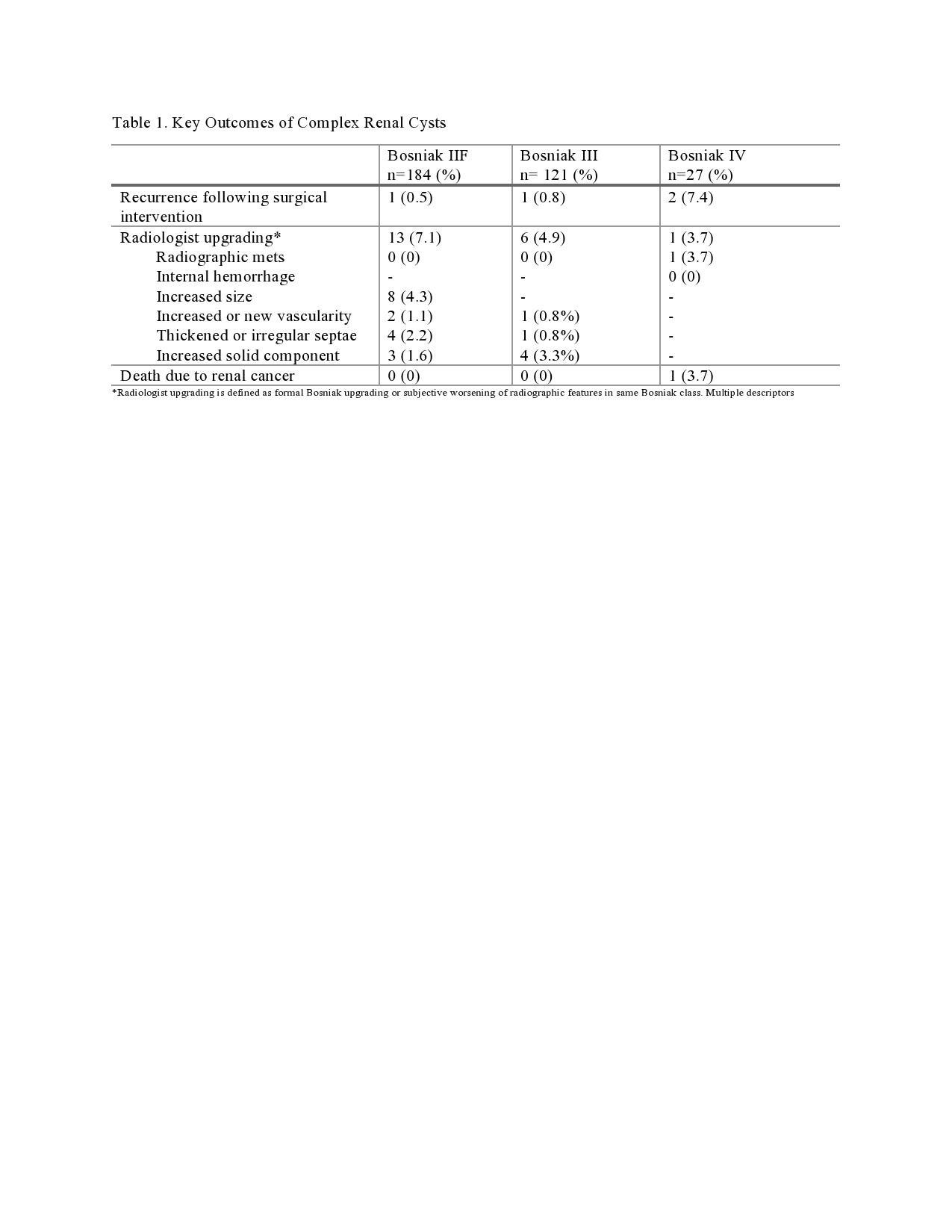
Introduction: The incidence of incidentally-detected renal cysts is high, ranging from 12% to 61%. While well-defined clinical consensus exists for Bosniak I and II renal cysts, our understanding of best practices for surveillance and management of complex renal cysts remains contended. This study aimed to evaluate key patient and disease-specific outcomes of complex renal cysts across an updated, twenty-year cohort. Methods: We performed a retrospective chart review of patients diagnosed with Bosniak IIF, III and IV renal cysts from 2001-2013 across three tertiary academic hospitals. Data from date of diagnosis to June 2022 was extracted, including demographics, cyst characteristics, biopsy and surgical/ablative intervention. Primary endpoints were radiologic upgrading (i.e. formal Bosniak upgrading or subjective worsening of radiographic features in same Bosniak class) and cancer-specific mortality. Results: A total of 332 patients with complex renal cysts were included: Bosniak IIF (55.4%, 184/332), Bosniak III (36.4%, 121/332), Bosniak IV (8.1%, 27/332). The majority of patients were male (63.3%, 210/332). Most patients were managed with active surveillance, except Bosniak IV patients where 66.7% (18/27) underwent upfront nephrectomy. Rates of biopsy were similar among Bosniak III and IV groups (22.3%, 27/121 and 22.2%, 6/27). Median follow-up for Bosniak IIF, III and Bosniak IV cysts on active surveillance was 7.8 years (IQR= 3.9-12.4yrs), 6.6 years (IQR= 3.7-10.1yrs) and 4.6 years (IQR= 3.7-8.6yrs), respectively. Twenty-eight percent of surgical patients (19/67) experienced peri-operative complications. The rate of radiologic upgrading for Bosniak IIF, III and IV was 7.1% (13/184), 4.9% (6/121) and 3.7% (1/27), respectively (Table 1). Cancer-specific mortality remained at 0.3% (1/332). Conclusions: Overall, despite lengthy follow-up, the rate of radiologic progression and cancer-specific mortality for complex renal cysts remains low. This analysis challenges conventional views of upfront intervention, particularly for Bosniak III cysts. It appears safe to de-intensify surveillance for complex renal cysts along with transfer of care to primary care providers (with appropriate direction and triggers for re-referral), especially for patients with compatible goals of care. SOURCE OF Funding: None

 photo")