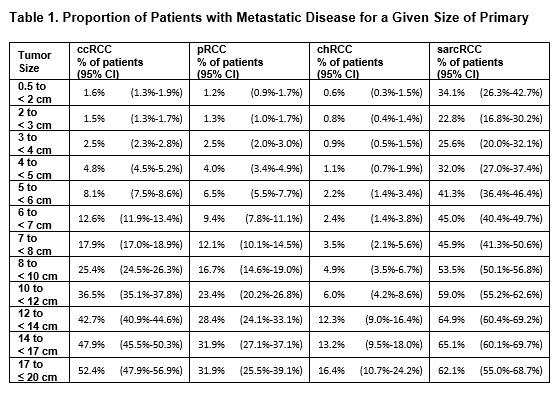
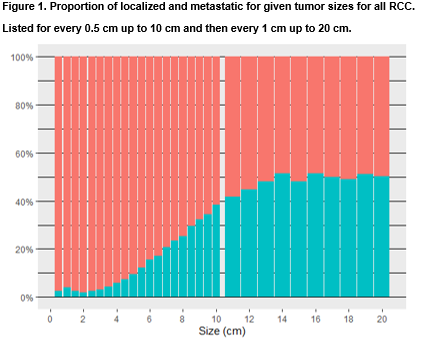
Introduction: Current data on the association between tumor size and metastases, and thresholds for intervention, for renal masses are largely based on single center nephrectomy registries. We sought to assess tumor size and metastatic status at presentation for patients with any RCC and for specific histologies using a cancer registry. Methods: Using SEER data we identified patients with a diagnosis of renal cell carcinoma made between 2004-2019. We assessed nodal and metastatic staging to identify non-localized disease. We performed specific assessments on clear cell (ccRCC), papillary (pRCC), and chromophobe (chrRCC) as well as RCC with sarcomatoid features (sarcRCC). We also assessed grade for ccRCC and pRCC. We report proportion of non-localized disease at various sizes and use logistic regression to establish statistical significance. Results: Of 181,096 patients with RCC included, 23,829 has non-localized disease. For RCC, any histology, 3 to 4 cm, 6 to 7 cm, and 10 to 12 cm tumors had non-localized rates of 4.0%, 16.7%, and 40.3% respectively. For chRCC non-localized rates were low at even large sizes. In contrast, sarcRCC had high non-localized rates at all sizes. ccRCC and pRCC non-localized rates increased steadily across each centimeter evaluated. For any RCC and each evaluated histology, tumor size was found to be associated with non-localized disease on logistic regression while controlling for sex; the odds ratio for each additional centimeter was 1.38, 1.29, 1.24, and 1.12 for ccRCC, pRCC, chRCC, and sarcRCC respectively (p < 0.001) . Conclusions: The likelihood of a small renal mass being metastatic varies greatly with both its histology and size. We report roughly twice the likelihood of non-localized disease across all tumor sizes compared to what has been reported previously in nephrectomy registries. These results may help clinicians pick appropriate thresholds for intervention and candidates for active surveillance, especially in those characterized by biopsy. SOURCE OF Funding: none