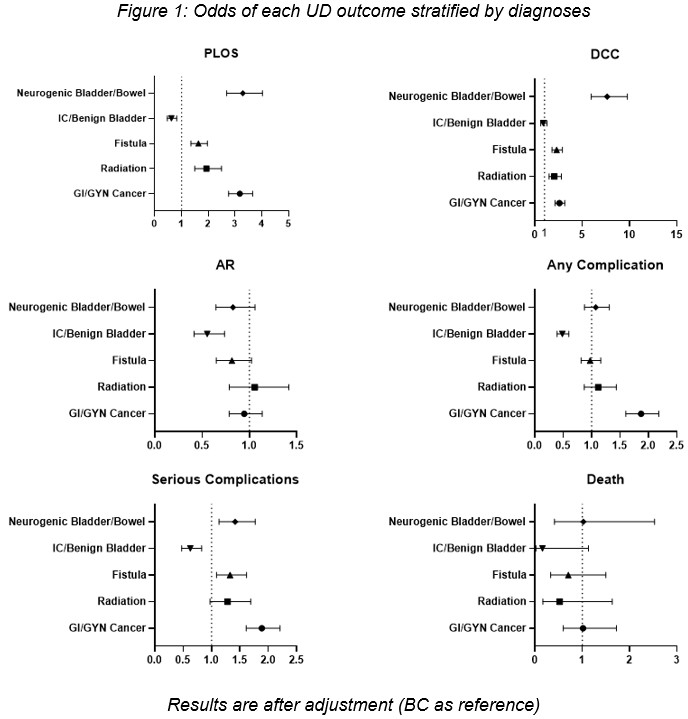
Introduction: Bladder cancer urinary diversion (UD) outcomes remain the benchmark to which all other UD are compared. However, a sizable proportion are done for other invasive cancers or benign etiologies of the bladder. There is a paucity of literature comparing outcomes of UD for various indications, both benign and malignant. Herein, we aim to compare health care utilization and 30-day morbidity among benign and malignant UD etiologies. Methods: Data were collected from the American College of Surgeons National Surgical Quality Improvement Program (ACS-NSQIP) from 2005-2020 on adult patients who underwent UD for various indications. ICD codes were used to assign patients to the following categories: Bladder Cancer (BC), GI/GYN Cancer (GC), Radiation (R), Fistula (F), Interstitial Cystitis/Benign Bladder (IB), and Neurogenic Bladder/Bowel (NGB). Patients that did not fall into these categories were excluded. Baseline characteristics and The Five Item Frailty Index (FFI) were compared across the 6 groups. Univariate and multivariate risk-adjusted regression models were developed to identify predictors of morbidity (30-day complications and mortality) and healthcare utilization (HU): prolonged length of stay (PLOS), 30-day readmissions (AR), and discharge to continued care (DCC). Results: A total of 22,534 patients met inclusion criteria. The majority had primary bladder cancer (88%), were males (79%), with a median age of 69. GC had the highest complication rate (64%) and PLOS (44%), R had the highest readmission rate (24%), while NGB had the highest DCC (29%). GC and IB were the least frail (˜ 14% with FFI=2) while NGB were the frailest (29%, p<.05). After adjusting for baseline characteristics (BC reference), there was a significant difference in PLOS, DCC, AR, and 30-day complication rates among different etiologies (p <.05, Figure 1). There was no significant difference in 30-day mortality. Compared to those with BC, those with NGB, F, R, and GC had significantly greater risk of serious complications and HU, whereas those with IB had a lower risk (p <.05). Conclusions: Postoperative HU and morbidity are greatly influenced by UD etiology. Care management in these vulnerable patient populations requires an individualized etiology-centered approach and cannot be benchmarked against those undergoing BC UD. SOURCE OF Funding: None

 photo")