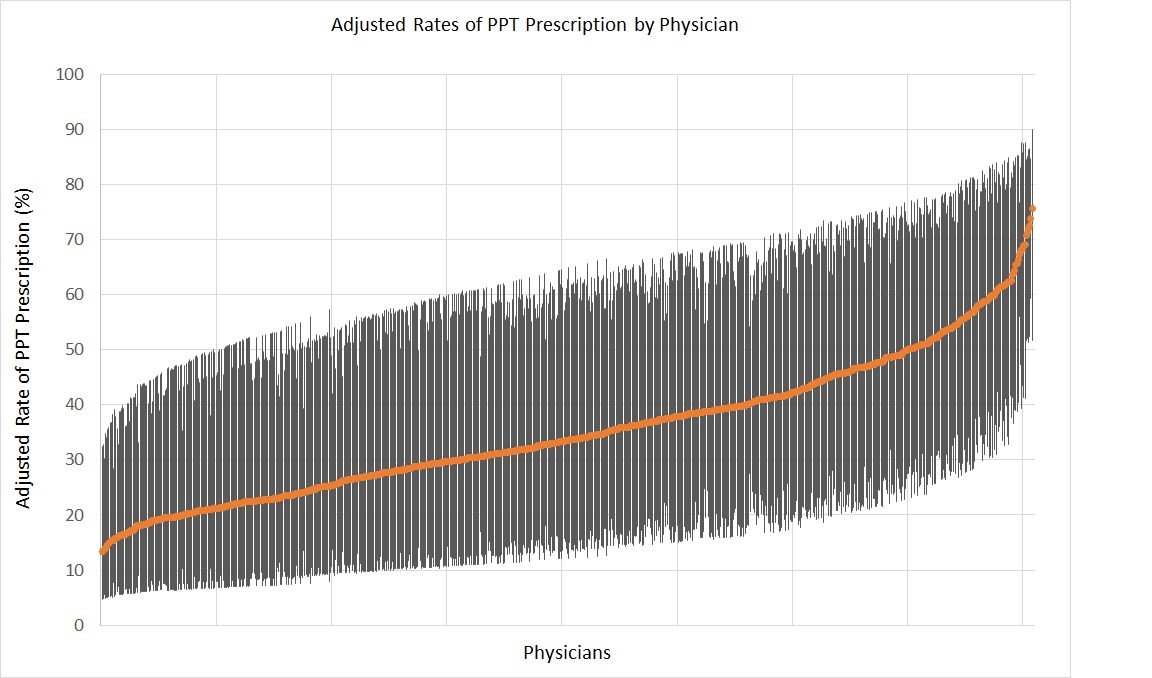
Introduction: Despite multiple clinical trials showing thiazide diuretics, alkali citrate therapy, and uric acid reducing agents (collectively referred to as preventive pharmacological therapy [PPT]) can lower the risk of kidney stone recurrence, these medications are infrequently prescribed. To better understand the barriers to PPT use, we analyzed a novel linkage of medical claims and urine chemistry data from a large cohort of patients with kidney stones. Methods: We identified Medicare beneficiaries with kidney stones with a 24-hour urine collection processed by Litholink from 2011 to 2016. Among the subset with an abnormal urine chemistry (hypercalciuria, hypocitraturia, hyperuricosuria, or low urine pH), we determined whether they had a prescription fill for PPT within six months of their collection. We characterized differences between patients who were prescribed PPT and those who were not. After assigning patients to the providers who ordered their urine collection, we fit multilevel models to determine how much of the variation in PPT prescription was due to patient- versus provider-level factors. Results: A total of 13,368 patients had a 24-hour urine collection with one or more abnormal urine chemistries, and 35.1% were prescribed PPT. Patients who were prescribed PPT tended to be younger, were more likely to be dually eligible for Medicare and Medicaid and had higher levels of comorbid illness (P <0.01). Eighteen percent of the variation in PPT prescription was attributable to the provider whom a patient saw. The Figure shows prescribing rates for 808 providers in the cohort, who saw 5 patients or more, which ranged from 13% to 76%. After accounting for patient characteristics and provider volume, patients had twice the odds of being prescribed PPT if they were cared for by a nephrologist (OR, 2.11; 95% CI, 1.79 to 2.49) or primary care physician (OR, 1.95; 95% CI, 1.38 to 2.75) versus a urologist. Conclusions: These data highlight that the type of provider patients see for their kidney stones is an important determinant of PPT prescription. As such, efforts to increase PPT uptake might include educational interventions targeting urologists. SOURCE OF Funding: Dr. Hollingsworth's research is funded by a grant from the National Institute of Diabetes and Digestive and Kidney Diseases R01DK121709.