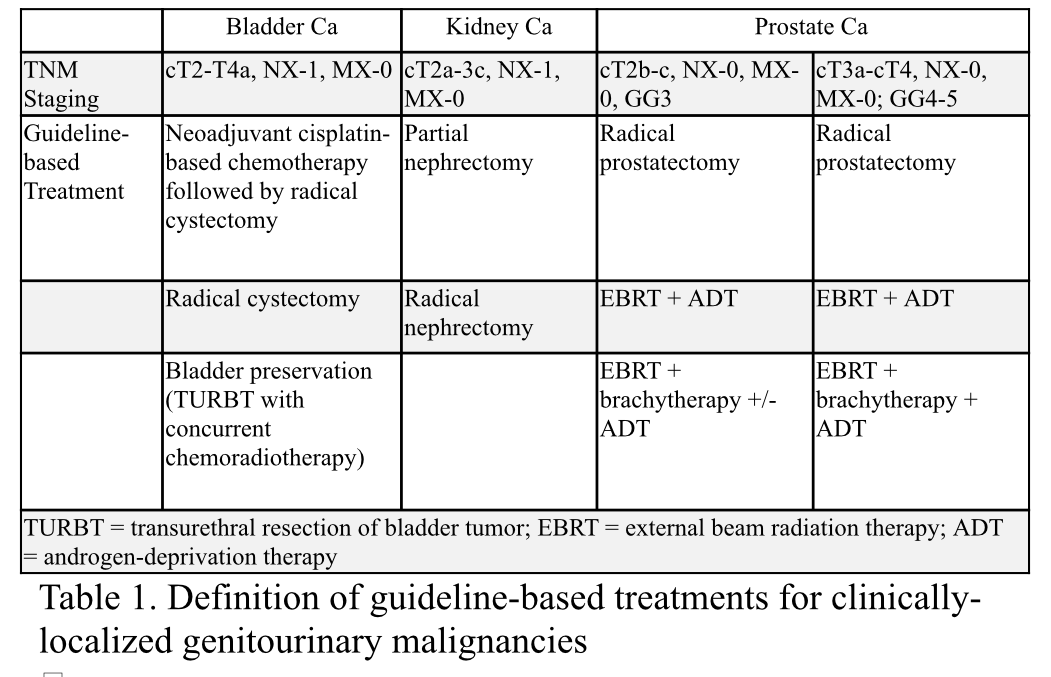
Introduction: Disparities in guideline-based treatment (GBT) for genitourinary cancers are commonly presented individually, impeding comprehensive examinations by of institutional drivers. Using GBT as a proxy for the quality of urologic cancer care received, we aim to characterize the prevalence of disparities in GBT for prostate (PCa), bladder (BCa), and kidney (KCa) cancer within the same facility to evaluate whether disparities cluster at the institutional level. Methods: Patients diagnosed with clinically localized bladder, prostate, or kidney cancer between 2004-2017 within each National Cancer Database dataset were included. We collected clinicodemographics, treatment received, and facility data. GBT was defined according to NCCN Guidelines by TNM staging [Table 1]. We calculated rates of GBT by cancer type and race and compared rates between White, Black, Hispanic, and Asian patients using Chi-squared tests. Pairwise correlations in GBT rates between PCa, BCa, and KCa treated across and within facilities were estimated using Pearson correlation coefficients, where facilities with <10 cases of each cancer were excluded. Results: We identified 91904 BCa, 73,050 KCa, and 252,403 PCa cases. BCa GBT was highest for White and Asian patients (50.5% and 48.6%, respectively) versus 42.2% for Black patients. KCa GBT rates were equivalent for White, Hispanic, and Asian patients (~76%) but lowest for Black patients (74.8%). In PCa, the highest GBT rate was 80.8% (White patients) and lowest was 76.5% (Black patients). After controlling for confounding variables and matching based on cohort size, intra-facility odds of receipt of GBT by Black patients (compared to White counterparts) correlated poorly across cancer types for all comparisons. This was true even when restricting analysis to higher-volume facilities (>200 patients), with r=0.1 for bladder-kidney, 0 for bladder-prostate, and 0.12 for kidney-prostate; p-value >0.05. Correlation coefficients at academic medical centers were highest among the four facility types, though still low (e.g., r=0.31 prostate-bladder). Conclusions: Our findings show that higher quality of care may cluster in a small proportion of facilities, but overall there is little correlation between disparities in GBT across GU cancers and race treated in the same facility. SOURCE OF Funding: UCSF