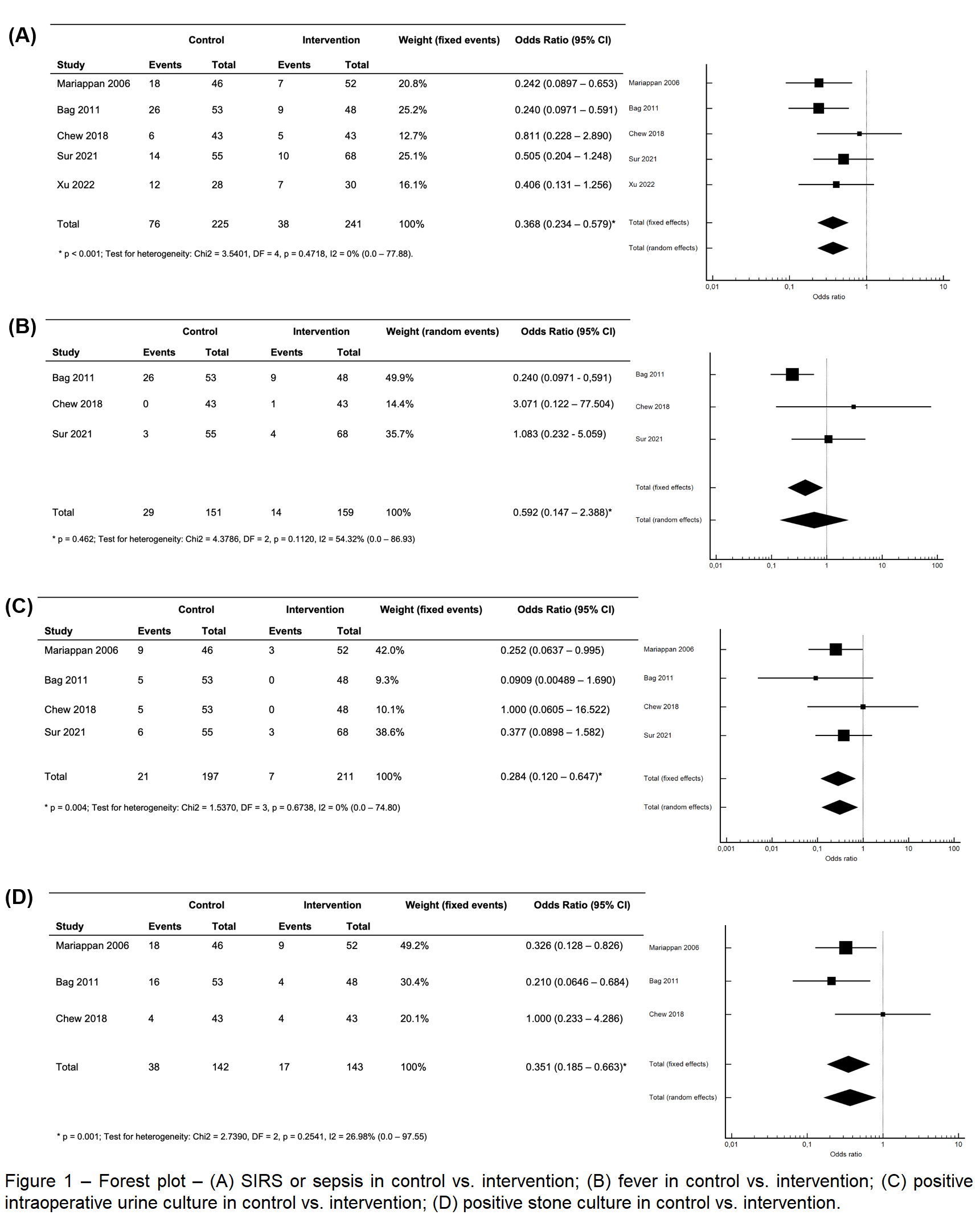
Introduction: Approximately 0.5% of the patients develop postoperative sepsis after percutaneous nephrolithotomy (PCNL). The aim of this study is to perform a high quality meta-analysis using only prospective studies to define the role of preoperative antibiotics in patients undergoing PCNL. Methods: This review was conducted according to PRISMA (preferred reporting items for systematic reviews and meta-analyses) statement. We selected prospective studies and randomized controlled trials that compared extended to short dose preoperative antibiotic prophylaxis in patients undergoing PCNL. A search for "percutaneous nephrolithotomy" and "antibiotic" was performed on EMBASE, PubMed and Web Of Science platforms, resulting in 1362 publications. The PICO (population, intervention, control and outcome) was: Population - adult patients that underwent to PCNL; Intervention - extended dose preoperative antibiotic prophylaxis before PCNL; Control - short dose preoperative antibiotic prophylaxis before PCNL; and Outcome: systemic inflammatory response syndrome (SIRS) or sepsis, fever after PCNL and positive intraoperative urine culture and stone culture. The meta-analysis protocol was registered on PROSPERO database (CRD42022359589). Alpha risk was defined as < 0.05. Results: The final selection was five articles with a total of 475 patients studied. Forest plots (figure 1) evidenced that using antibiotics for 7 days in preoperative period of PCNL was a protective factor for developing SIRS/sepsis (OR 0.366, 95% CI 0.234 - 0.527, p < 0.001). There was no statistical association between seven-day use of antibiotics and fever (OR 0.592, 95% CI 0.147 – 2.388, p = 0.462). Patients who received intervention had lower positive intraoperative urine culture (OR 0.284, 95% CI 0.120 – 0.674, p = 0.004) and stone culture (OR 0.351, 95% CI 0.185 – 0.663, p = 0.001) than control group. Conclusions: We conclude that one week of prophylactic oral antibiotics based on local bacterial sensitivity pattern in patients undergoing PCNL reduces the risk of infection. SOURCE OF Funding: None.

.jpeg.jpg "Thalita Bento Talizin, MD,MSC photo")