CRTA Post-Doctoral Research Fellow, Urologic Oncology Branch, National Cancer In
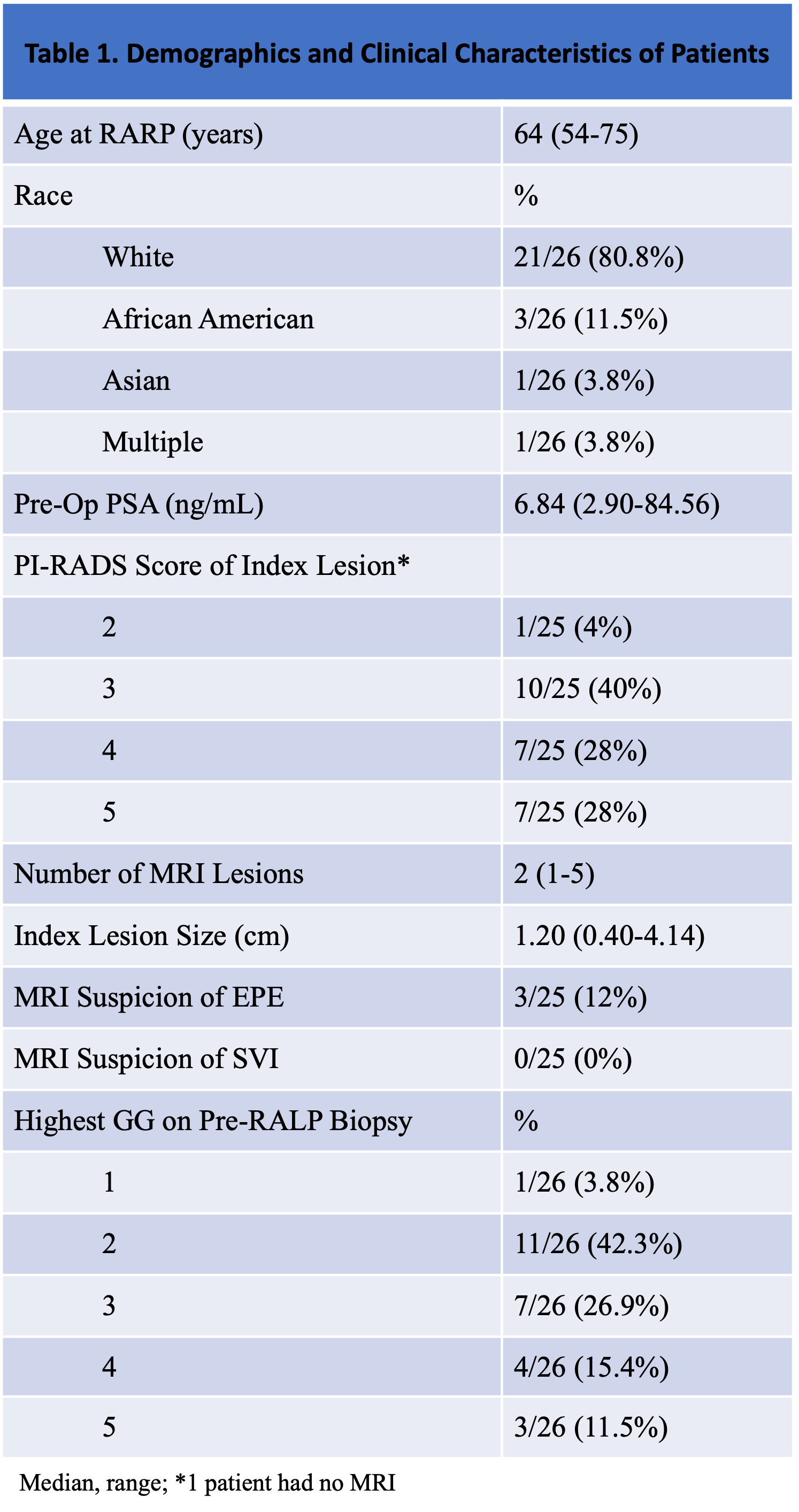
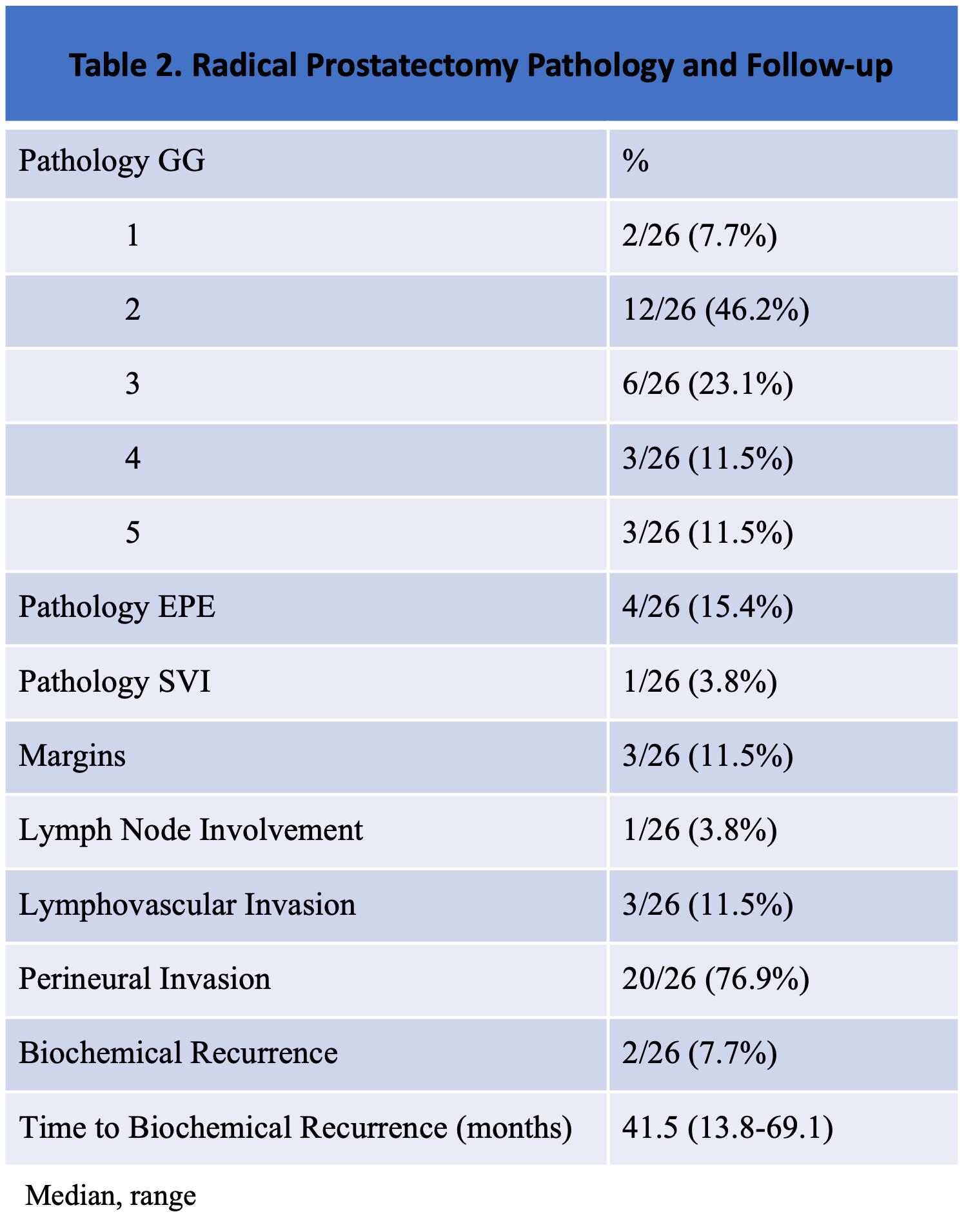
Introduction: PROSTVAC is a therapeutic cancer vaccine designed to activate T cells specific against prostate-specific antigen (PSA). Previous trials have shown PROSTVAC to be safe and capable of modulating immune responses in patients with localized prostate cancer (PCa). We aim to examine the surgical safety and feasibility outcomes of patients in a phase II trial (NCT02153918) investigating the neoadjuvant use of this vaccine therapy in patients with localized PCa. Methods: An open-label, phase II study of neoadjuvant PROSTVAC vaccine enrolled patients with histopathologically confirmed localized PCa who were surgical candidates for radical prostatectomy (RP). Patients received recombinant vaccinia (rV)-PSA(L155)-TRICOM (PROSTVAC) as a priming vaccination, followed by monthly boosts on weeks 5, 9 and 13 with recombinant fowlpox (rF)-PROSTVAC. The boosting schedule was amended mid-trial to weeks 3, 5 and 9 to allow for earlier surgeries. After completing the vaccination series, patients underwent RP at week 10. Final follow-up safety evaluation was performed 12–15 months postoperatively. Results: Between 2014-2016, 26 of 27 enrolled patients went on to receive RP. On pre-RP biopsy, 12/26 (46.2%) of patients had Gleason grade group (GG) 1-2, and 14/26 (53.8%) of patients had GG 3-5 (Table 1). Two patients (7.7%) were upgraded, and five (19.2%) downgraded on final pathology. Rates of adverse features at RP are shown in Table 2. The most common adverse event (AE) was a self-limited injection-site reaction (28 events in 18 patients), and no serious AEs or toxicities > grade 2 were attributed to PROSTVAC. However, two grade 3 serious AEs occurred: an infected lymphocele and a thromboembolic event, both attributed to surgery. Conclusions: PROSTVAC was well tolerated and demonstrated the feasibility of neoadjuvant vaccination strategies for localized PCa. Further studies will be needed to elucidate the effectiveness of this vaccine therapy on short and long-term oncologic outcomes. SOURCE OF Funding: NIH intramural research program