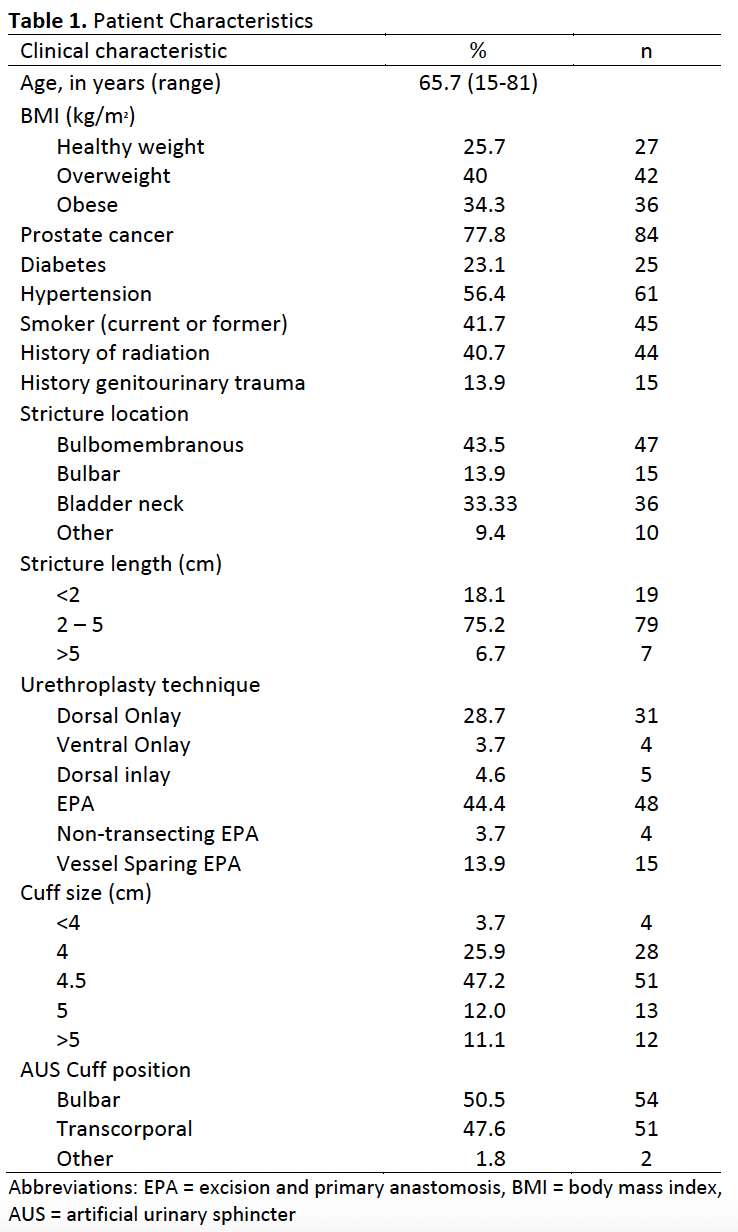
Introduction: The artificial urinary sphincter (AUS) is generally accepted as the gold standard for male stress urinary incontinence (SUI). There is limited and conflicting evidence on outcomes when urethroplasty precedes AUS insertion, and even less scrutiny of whether and how urethroplasty technique affects these outcomes. We sought to evaluate complications of AUS insertion after urethroplasty in a multi-institutional cohort. We hypothesize that complications occur at higher rates in this population and vary between augmentation and anastomotic urethroplasty. Methods: 108 patients were identified who underwent AUS after urethroplasty. Demographic and clinical variables were analyzed. Urethroplasties were categorized as either transecting or non-transecting. Long term complications included AUS infection, erosion, and mechanical failure. Analysis was performed using Stata/BE 17.0. For descriptive statistics, continuous variables were presented as the mean or median and categorical variables were presented as absolute numbers and percentages. Chi squared test was used for categorical variables. Tests performed were two-sided and p < 0.05 was considered to indicate statistical significance. Results: 108 cases were identified that were performed by 13 surgeons (range 2-26). Characteristics of the sample are included in Table 1. Long term AUS complication risk including AUS infection, erosion, and mechanical failure following transecting urethroplasty was 53% compared to 29% following non-transecting urethroplasty (p = 0.01). Among 59 patients who had non-transecting urethroplasty, 10 experienced erosion, 3 infection, and 3 mechanical failure. Among 49 patients who had transecting urethroplasty, 16 experienced erosion and 10 mechanical failure. Median follow-up was 30 months following AUS insertion. Conclusions: For patients undergoing AUS insertion after urethroplasty, complications occur at higher rates than outcomes in the general population. Patients who undergo transecting urethroplasty are twice as likely to experience AUS complications compared to patients who had undergone non-transecting urethroplasty. Non-transecting urethroplasty may be advisable if a subsequent need for AUS is anticipated. SOURCE OF Funding: N/a