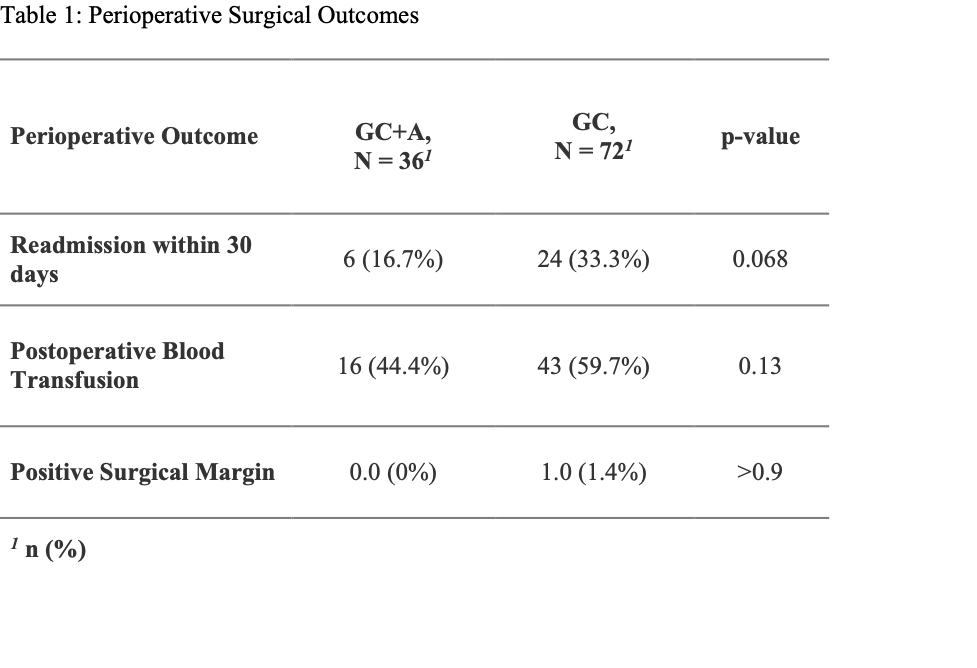
Introduction: Safety and efficacy were reported in the multicenter phase II trial of neoadjuvant gemcitabine, cisplatin (GC), and atezolizumab (A) therapy in patients with muscle-invasive bladder cancer (MIBC) (Funt et al., JCO 2022). Adding A to GC resulted in a 69% downstaging of MIBC ( Methods: Patients who underwent RC after neoadjuvant GC+A in the trial were matched using 2:1 nearest neighbor matching to a contemporary cohort of 72 patients who received neoadjuvant GC followed by RC from February 2018 to May 2020 at Memorial Sloan Kettering Cancer Center. Patients were matched on BMI, age-adjusted Charlson comorbidity index, surgical approach, ASA score, clinical stage, and smoking status. Surgical outcomes were assessed between treatment groups using Wilcoxon Rank Sum or Fisher’s Exact tests. To adjust for remaining differences, treatment coefficients were estimated using logistic regression models for categorical outcomes and linear models for continuous outcomes, stratified on propensity score quartiles. Results: The cohort's median age was 67 (range 37 – 80). The cohort was predominately male (75%) with clinical stage T2 or lower (79%). Perioperative surgical outcomes were not significantly different between both groups (Table 1). Logistic regression models, stratified by propensity score quartiles, revealed no association between the treatment type and postoperative transfusion (OR: 0.52, 95% CI: 0.22 – 1.23) or readmission within 30 days (OR: 0.57, 95% CI: 0.20, 1.62). Grade 3 or above adverse events rate in both the GC+A and the GC groups was 19.4% and 22.2%, respectively (p = 0.7). Conclusions: The addition of neoadjuvant atezolizumab to the gemcitabine/cisplatin regimen for patients with MIBC undergoing RC did not result in significantly higher perioperative complications compared to a contemporary group of patients receiving GC alone. SOURCE OF Funding: Clinical trial information: NCT02989584. Research Sponsor: Genentech, Inc, U.S. National Institutes of Health.