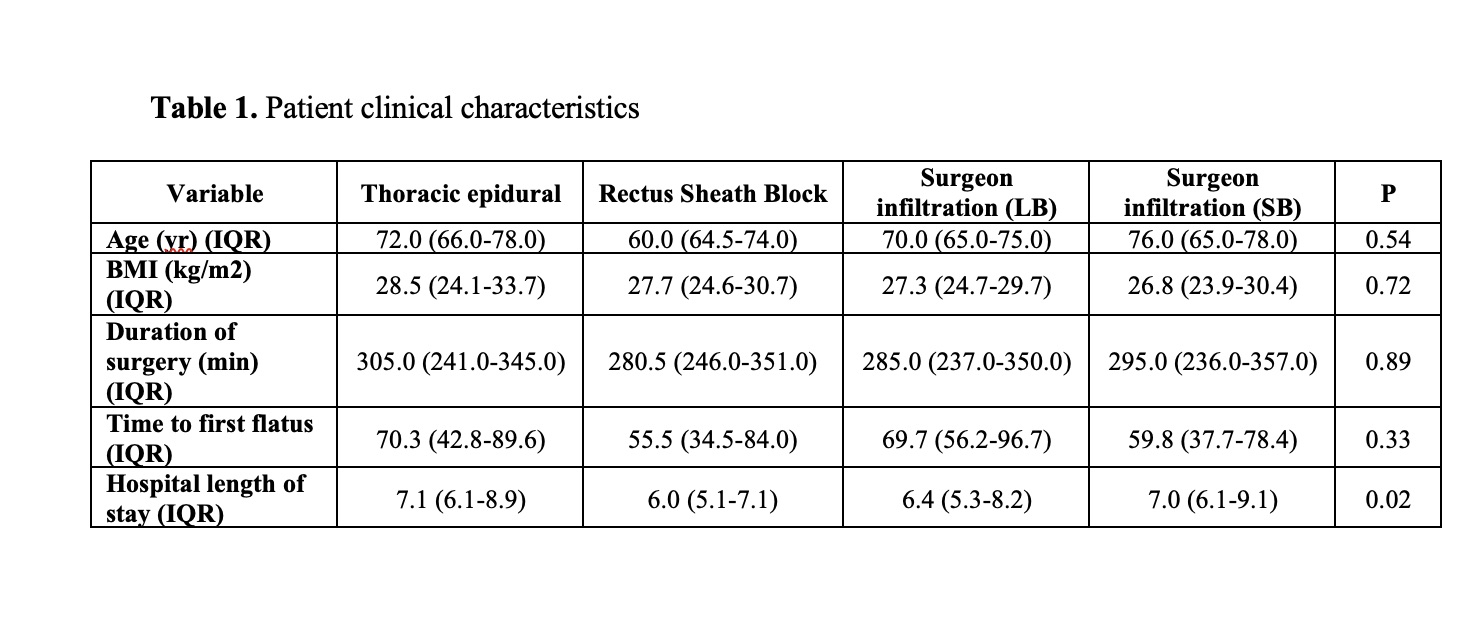
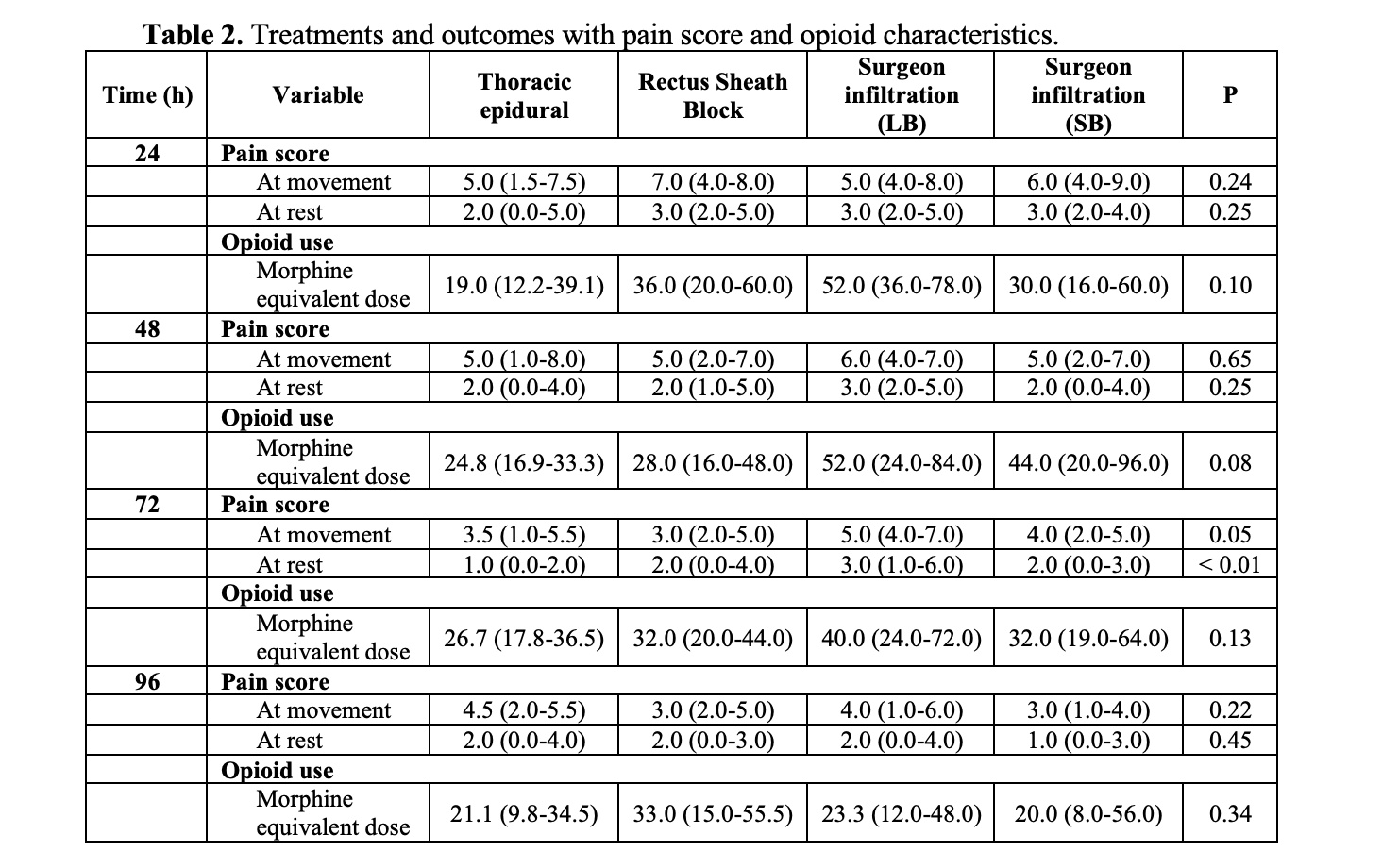
Introduction: Enhanced Recovery After Surgery (ERAS) protocols have been increasingly implemented for perioperative care. Radical cystectomy with urinary diversion can have significant morbidity with analgesic control and return of bowel function. Our aim was to prospectively study the best perioperative pain regimen between thoracic epidural anesthesia (TEA), rectus sheath block (RSB), and surgeon infiltration (SI) with liposomal bupivacaine (LB) or standard bupivacaine (SB). Methods: All patients were prospectively scheduled at Indiana University for cystectomy with diversion and randomized into four groups – TEA with bupivacaine/hydromorphone, RSB with LB, or SI with LB or SB. Visual Analog Scale (VAS) pain scores, opioid use, incidence of hypotension, nausea, sedation was compared between groups every 24 hours as well as time to first flatus, hospital length of stay were measured. Analysis of Variance (ANOVA) and link function testing was performed to assess significance between groups, with an alpha value of 0.05. Results: We enrolled 160 patients with 40 in each group. Demographic and clinical characteristics are listed in Table 1 with no significant differences between groups. Table 2 lists outcomes of pain scores with no differences between regimens, although patients tended to use less opioids with a TEA (p=0.1 at 24 hrs, p=0.08 at 48 hrs, p=0.13 at 72 hrs, and p=0.34 at 96 hrs). Similar incidence of sedation, nausea, and hypotension were also seen between groups. Despite no significant difference with time to first flatus (p=0.32), length of stay was longer for patients with TEAs and shorter with RSB or SI with LB (p=0.02). Conclusions: In this randomized prospective study for perioperative pain control during radical cystectomy, TEA trended towards less opioid use whereas time to flatus and hospital length of stay was longer compared to RSB or SI. These various options may be tailored based on clinical scenario. Further studies may help improve all aspects of perioperative care to minimize morbidity. SOURCE OF Funding: None