Case Western Reserve University School of Medicine
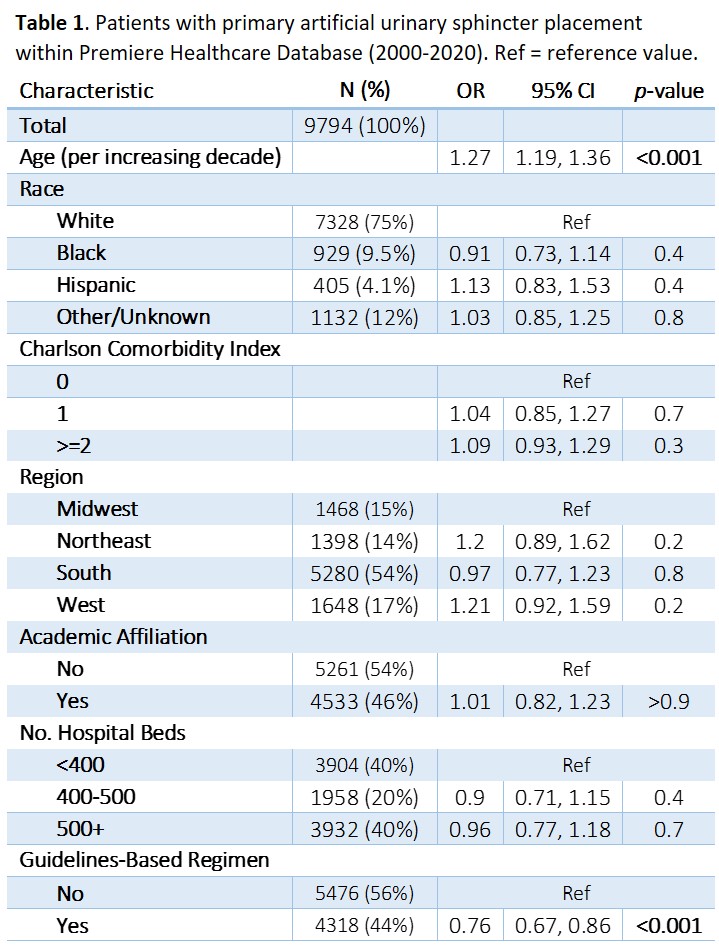
Introduction: Perioperative antimicrobial prophylaxis is crucial for prevention of patient morbidity after artificial urinary sphincter (AUS) placement. While antibiotic guidelines exist for urologic procedures, adoption patterns for AUS surgery are unclear. We aimed to assess trends in antibiotic prophylaxis for AUS and outcomes relative to American Urological Association (AUA) best practice statements. Methods: The Premier Healthcare Database was queried from 2000 to 2020. Encounters involving AUS insertion, removal, and/or associated complications were identified via ICD and CPT codes. Premier charge codes were used to identify antibiotics used during the insertion encounter. Guideline-based regimens were defined as 1) aminoglycoside (AG) + 1st/2nd generation cephalosporin (CEP), 2) AG + vancomycin, 3) aztreonam and CEP, 4) aztreonam and vancomycin, 5) aminopenicillin, or 6) beta-lactamase inhibitor. AUS-related complication events were found using patient hospital identifiers. Univariable analysis between hospital/patient characteristics and use of guideline-based antibiotics was done via chi-squared and Kruskal Wallis tests. A logistic regression model was used to determine the odds ratio (OR) of complications. Results: Of 9794 patients with primary AUS surgery, 4318 (44%) received guideline-based antibiotics. Probability of guideline-based regimen use increased 7.5% per year. Patients with guideline-based regimens had lower odds of any complication within 3 months vs. non-guideline regimens (OR 0.76, 95% CI 0.67-0.86); however, no significant difference in repair/removal was noted (OR 0.99, 95% CI 0.86-1.14). Each decade increase in age was associated with a 17% increase in complications (95% CI 1.11-1.24). No significant difference was noted with Charlson comorbidity index, region, or hospital size. Conclusions: Adherence to AUA antimicrobial guidelines for AUS surgery appears to have increased over time. Use of guideline-based regimens was associated with lower likelihood of complications, however they did not appear to lower surgical revision rates. SOURCE OF Funding: None