University of Alabama at Birmigham School of Medicine
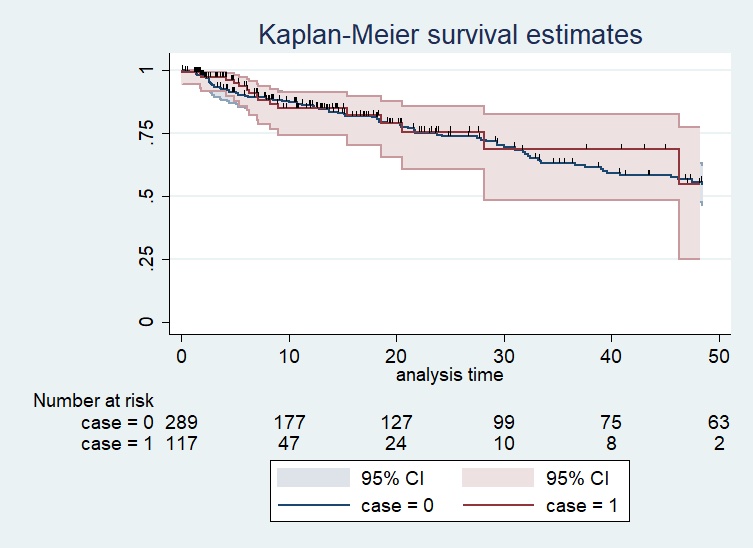
Introduction: Placement of an artificial urethral sphincter (AUS) for stress urinary incontinence may result in postoperative urinary retention. Therefore, patients often remain catheterized for a 23-hour period, despite a lack of evidence to support this practice. Our study aims to evaluate the feasibility of outpatient, catheter-free continence surgery using a multi-institutional database. We hypothesize that between catheterized controls and patients without a catheter, there would be no difference in rate of urinary retention or post-operative complications. Methods: We conducted an IRB-approved retrospective review of patients undergoing first-time AUS placement from 2009-2021. Patients were stratified by postoperative catheter status into either immediate decatheterization — leaving the procedure without a catheter — or controls — placement of an indwelling catheter for 23 hours. Data were collected on demographic and surgical variables from five institutions. The primary outcome, urinary retention, was defined as catheterization due to subjective voiding difficulty or documented PVR over 250 mL. Analyses were performed using STATA with p<0.05 considered significant. Results: Our study identified 302 controls and 123 immediate decatheterization. Twenty (6.6%) historic controls and nine (7.3%) immediate decatheterization patients developed urinary retention requiring short term catheterization (p=0.80). The immediate decatheterization cohort had a higher rate of complication (19.2% vs 33.3%), but there was no difference in the rate of urinary tract infections (UTI) (2.6% vs 2.4%, p=0.90), surgical site infections (SSI) (1.3% vs 2.4%, p=0.41), or device erosions between groups (1.7% vs 0.8%, p=0.51). Kaplan-Meier survival analysis revealed no significant difference in the rate of revision surgery (Figure 1). Conclusions: In our cohort, there was no difference in urinary retention, device erosion, UTI, and SSI rates between immediate intraoperative catheter removal and those catheterized for 23 hours. Early decatheterization enables outpatient incontinence surgery without altering reoperation over medium-term follow up. SOURCE OF Funding: None.

 photo")