Session: MP72: Health Services Research: Quality Improvement & Patient Safety II
MP72-01: A randomized controlled trial (RCT) of one-stage or a novel two-stage consent in men offered a brief mind-body intervention during prostate biopsy
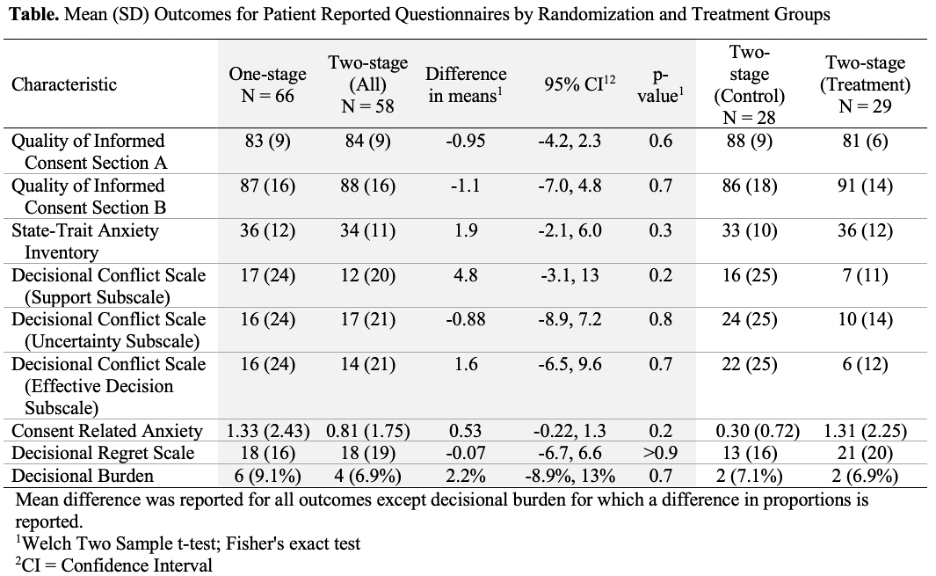
Introduction: Poor trial accrual caused by cumbersome informed consent procedures delays advancements in clinical medicine. Two-stage consents may improve patients’ informed consent experience by avoiding information overload, prioritizing patient treatment autonomy, and eliminating placebo regret. We tested the feasibility of enrollment and patient reported outcomes for two-stage consent in a “low stakes” RCT of a brief mind-body intervention during prostate biopsy (mindful biopsy). Methods: We performed a RCT of one stage (standard) or two stage (an initial consent indicating willingness to be approached for a randomized prostate biopsy intervention followed by a second consent for patients randomized to the intervention) consent as part of a RCT of mindful biopsy versus usual care (NCT03507725). We compared patient reported Quality of Informed Consent (QuIC), State-Trait Anxiety Inventory (STAI), Decision Conflict Scale (DCS), Consent Related Anxiety (CRA), and the Decisional Regret Scale (DRS) between groups. Differences in means and dichotomous variables were calculated using two-sample t-tests and Fischer’s exact tests, respectively. Results: Among 125 enrolled, 64/66 patients randomized to one-stage consent and 58/59 randomized to two-stage participated. 29/58 patients in the two-stage consent arm were randomized to treatment. There was no statistically significant difference in the QuIC and the 95% CI excludes any clinically relevant difference between patient understanding of one-stage and two-stage consent. Furthermore, STAI, DCS, CRA, and DRS and were similar between one and two-stage consent (Table). Although second stage consent was often conducted on the day of biopsy, CRA scores were similar between two-stage treatment and one-stage consents (1.3 and 1.3) and there was a signal toward improved anxiety in the two-stage control group (0.3). Conclusions: Robust patient enrollment in “low stakes” clinical trials is feasible using two-stage consent and maintains patient understanding of consent. Though unanticipated for this “low stakes” trial, we saw some evidence of lower anxiety from two-stage consent. Future studies should evaluate two-stage consent in trials with higher stakes. SOURCE OF Funding: PCORI