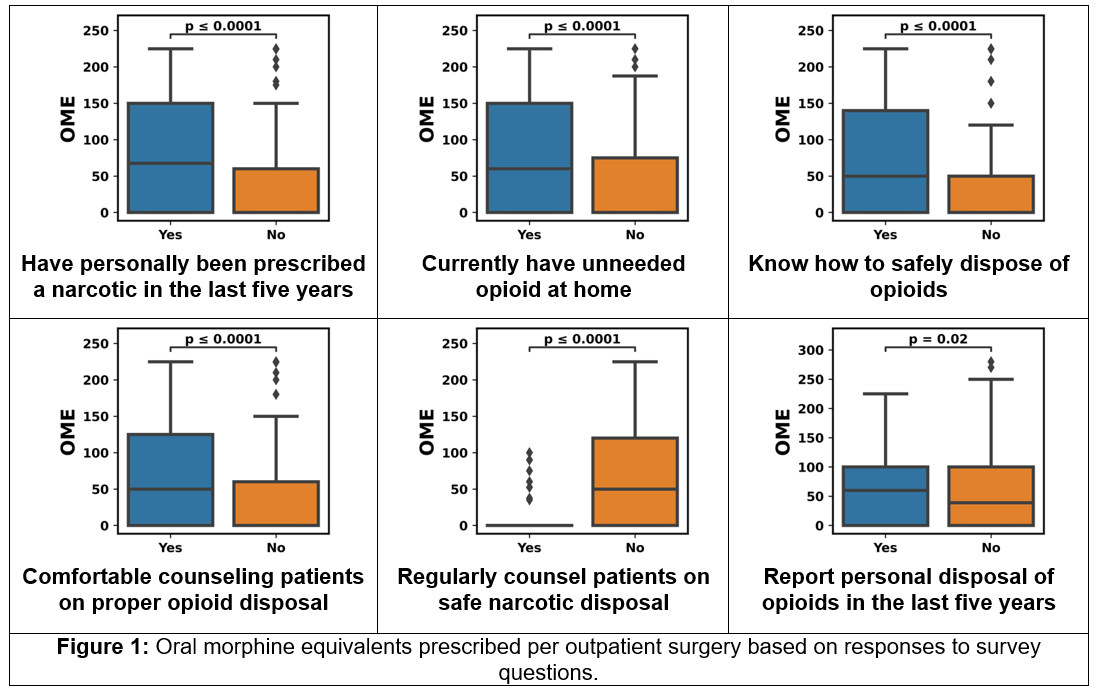
Introduction: Decreased unnecessary opioid prescribing has the potential to mitigate downstream population-level consequences. To our knowledge, no prior studies have evaluated how a physicians’ personal opioid use and storage influences prescribing. Methods: After IRB approval (MU #2015185), a Confidentiality Certificate (#CC-OD-19-483) was obtained. An online survey was distributed to all surgeons at our institution. The questionnaire focused on personal opioid use, disposal patterns, knowledge, and counseling habits. We then abstracted prescribing records after outpatient surgery for each surgeon and evaluated relationships using non-parametric tests and multivariate analyses. Results: The survey was completed by 30/98 (funding limit) surgeons. 47% had been prescribed opioids in the previous 5 years and 30% had unneeded opioids in their home. 73% knew how to dispose of opioids safely, 67% were comfortable counseling patients on this, but only 17% regularly counseled patients on disposal. Of 1989 procedures from August to October 2019, 671 were performed by a respondent. Multivariate analysis demonstrated that all survey questions and characteristics except patient race and provider age were correlated to the amount of opioid prescribed. Provider-specific factors associated with amount of opioid prescribed included provider gender, specialty, and opioid and non-opioid prescribing before and at discharge. Physicians with recent personal opioid prescription, unneeded opioids, and proper disposal knowledge were more likely to prescribe opioids and in greater amounts (Figure 1). Conclusions: We examined how physician personal opioid use, disposal, and knowledge impact prescribing after outpatient surgery. We found that a surgeon’s personal opioid use and disposal habits are risk factors for increased prescribing. This may represent a knowledge and modifiable risk factor for opioid overprescribing. SOURCE OF Funding: University of Missouri Department of Surgery