IRCCS Ospedale San Raffaele / Università Vita-Salute San Raffaele
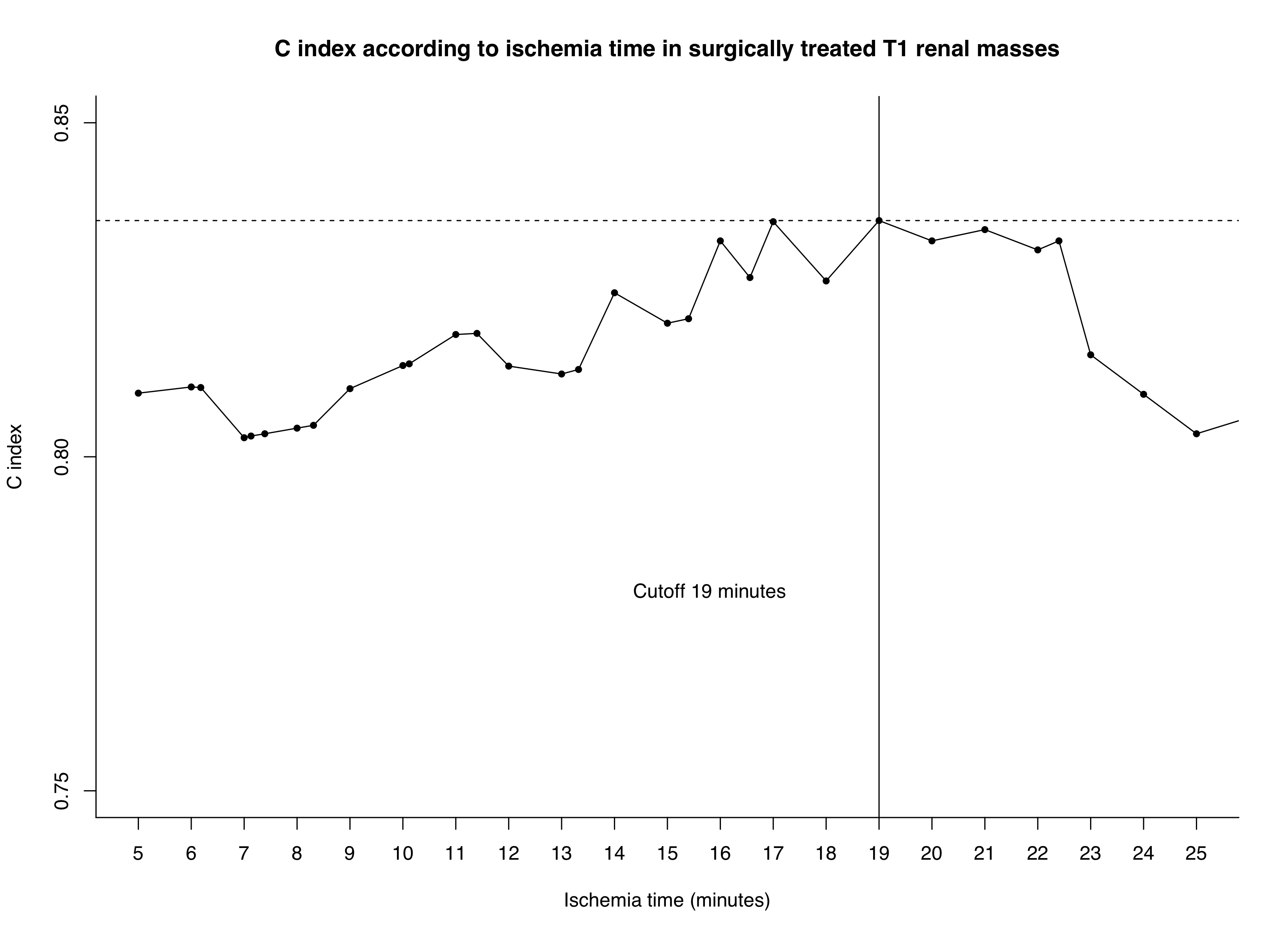
Introduction: Robot-assisted partial nephrectomy (RAPN) is the gold-standard treatment for T1 renal masses. To reduce bleeding, renal artery clamping is often required, and several cut-offs for the ‘safe’ duration of intraoperative warm ischemia time (WIT) have been proposed. However, due to the lack of systematic and detailed analysis, the optimal cutoff is still subject of significant debate. We aimed to identify the best WIT cut-off to predict acute kidney injury (AKI). Methods: We relied on 305 patients treated with RAPN between 2009 and 2020. All patients were treated by highly experienced surgeons. Patients undergoing clampless RAPN, as well as patients harbouring multiple masses, were excluded. The primary endpoint was AKI defined as a rise >0.3 mg/dL between pre- and post-operative creatinine or a 1.5-fold higher value of creatinine at discharge as compared to baseline creatinine. Multivariable Cox regression models examined the impact of WIT on AKI after adjustments for age, sex, pre-operative creatinine, solitary kidney, chronic kidney disease, clinical tumor size and PADUA score. The C-index was used to identify the WIT cut-off with highest accuracy. Results: Median age was 63 years (interquartile range [IQR]: 54, 71) and the majority of patients were male (197, 67%). 15 (5%) patients had a solitary kidney, 17 (6%) harbored chronic kidney disease, while median pre-operative creatinine was 0.9 mg/dL (IQR: 0.8, 1.0). Median tumor size was 3.1 cm (IQR: 2.0, 4.3) and median PADUA score was 8 (IQR: 7, 10). Median WIT time was 14 minutes (IQR: 10, 18). Overall, 47 (15%) patients experienced AKI before discharge. On multivariable Cox regression models, all variables with the exception of PADUA score, represented independent predictors of AKI (all p<0.05). The WIT cut-off associated with the highest accuracy in predicting AKI was 19 minutes (C-index: 83.5%). When individuals were stratified according to the 19 minutes cut-off, AKI was present in 12% vs 28% of those with an WIT time below vs. above the threshold (Figure 1). Conclusions: Consensus for appropriate duration of ischemia during RAPN for T1 renal masses is lacking. Here, we performed detailed and systematic cut-off analyses of WIT and identified an optimal cut-off of 19 minutes. SOURCE OF Funding: None

 photo")