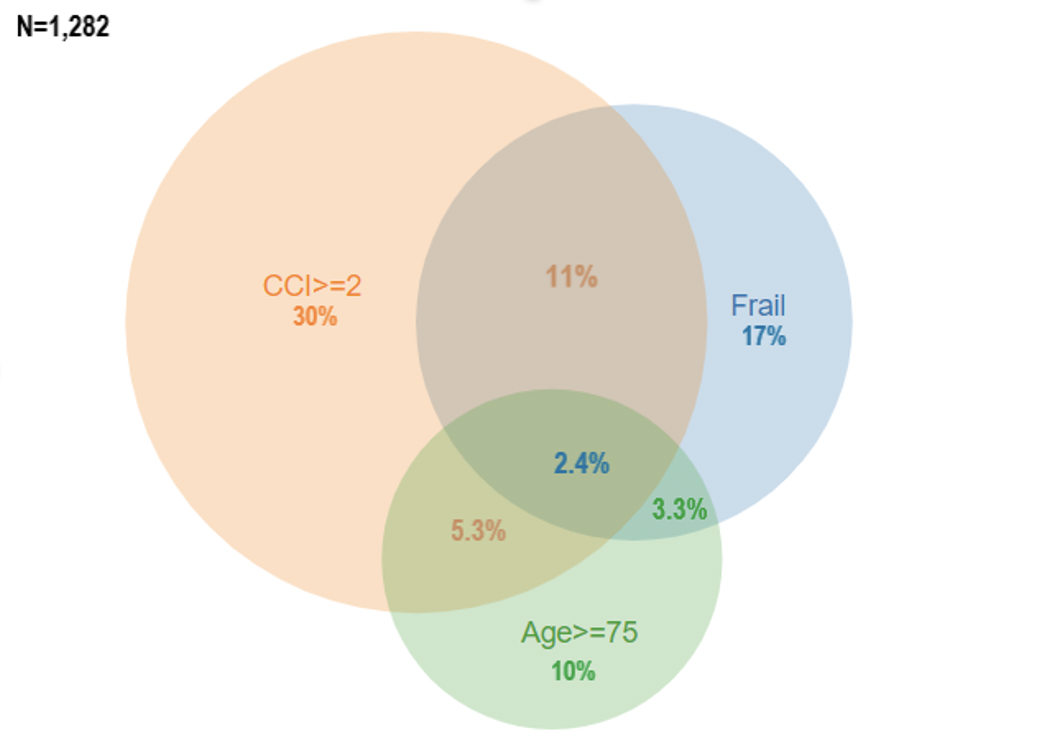
Introduction: Partial nephrectomy (PN) is the gold standard treatment for localized renal cell carcinoma (RCC), when technically feasible. However, PN is not devoid of complications. We investigated the role of the National Surgical Quality Improvement Program – Frailty Index (NSQIP-FI) on postoperative outcomes in patients undergoing PN for RCC. Methods: We relied on a prospectively maintained database including 1,282 patients treated with PN for cT1-2 RCC. The NSQIP-FI score was used to identify frail patients. Prolonged length of stay (pLOS) was defined as LOS above the median. Venn diagram was used to graphically depict the rate of frailty, Charlson Comorbidity Index (CCI) >2 and age >75.Three separate multivariable logistic regression models (LRM) were built to test the impact of frailty status, CCI and age on postoperative complications and pLOS, respectively, after adjusting for patient and tumor characteristics. Finally, area under the curve (AUC) was calculated after including the NSQIP-FI score within the postoperative models predicting complications and pLOS. Results: Of 1,282 patients, 220 (17%) were frail according to NSQIP-FI, 391 (30%) had CCI >2 and 134 (10%) were older than 75 years. Median BMI and clinical size were 25 [Interquartile range (IQR): 23-28] kg/m2 and 3 (IQR: 2.4-3.7) cm. Median LOS was 4 (IQR: 3-5) days. The overall rate of complications was 27%, and 4% with Clavien-Dindo >2. At MVA, after confounders, frailty status represented the strongest predictor of postoperative complications [Odds ratio (OR): 1.45, p<0.01], compared to CCI >2 (OR: 1.28, p=0.01) or age >75 (OR: 1.36, p<0.01). Moreover, when NSQIP-FI was included into the postoperative models predicting complications, the AUC increased from 76 to 82%. The same phenomenon was observed relative to prolonged LOS (AUC from 72 to 79%). Conclusions: The rate of frail patients undergoing PN is higher than elderly patients (>75 years). Moreover, the NSQIP-FI does represent the strongest predictor of adverse outcomes after surgery, namely overall complications and pLOS. In consequence, preoperative assessment of NSQIP-FI allows for a better stratification of surgical risks in patients candidate to kidney surgery and for selecting those patients which may deserve a dedicated geriatric assessment. SOURCE OF Funding: None