Session: MP58: Kidney Cancer: Localized: Surgical Therapy III
MP58-19: Detection of pulmonary lesion during follow-up after surgery for localized renal cell carcinoma: disease progression or a primary lung cancer?
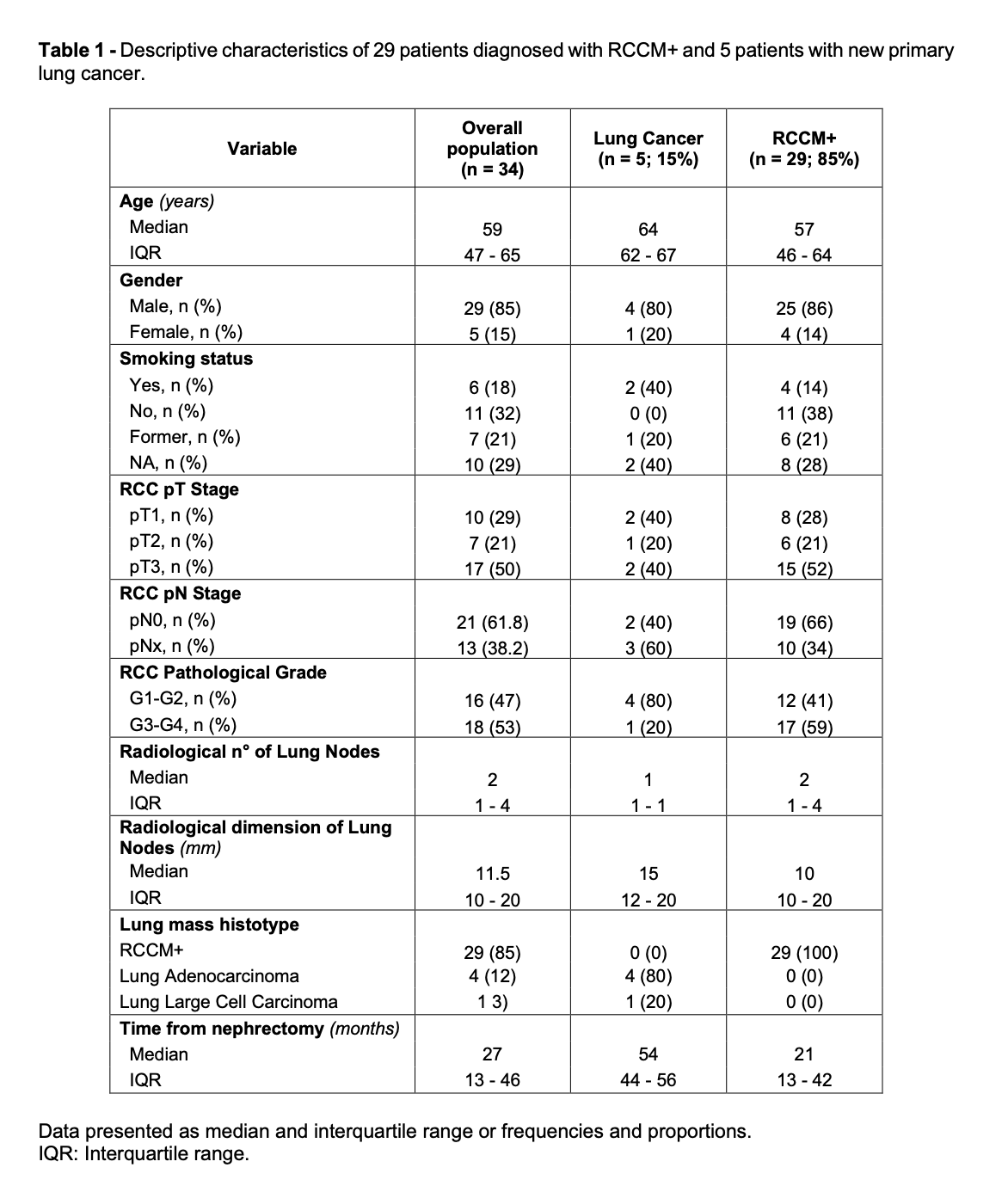
Introduction: The lung is the most common anatomical location in case of renal cell carcinoma metastasis [RCCM+] after surgery. However, not all the pulmonary masses recorded at follow-up are RCCM+, since some patients can develop primary lung cancer [LC] during follow-up, as well. The aim of the study was to define the rate of metachronous lung cancer in patients with suspected lung metastasis after a previous treatment for RCC and to investigate the possible differences in clinical and radiological features. Methods: From a prospectively maintained database, we collected detailed information regarding 81 patients treated with surgery for cM0 RCC who presented with a pulmonary mass at CT during follow-up. The primary outcome of the study were the rates of RCCM+ and LC defined with fine needle aspiration for diagnostic purpose or pathology after surgical resection for therapeutic purpose. Clinical, radiological, and histopathological features RCCM+ and LC were scrutinized as secondary outcomes. Results: In 42% of the study population, histological diagnosis of the lung mass was available. The rate of RCCM+ was 85% and the rate of LC was 15%. Despite the study sample size does not allow for formal statistical inference, some differences in the clinical, radiological, and histological features of RCCM+ and LC patients deserve consideration (Fig. 1). Relative to patients with RCCM+, who were more likely to have multiple nodules, all patients with LC had a single mass. Similarly, relative to patients with RCCM+, patients with LC had a larger mass, were more likely to have history of smoking, to have a less aggressive RCC primary and a longer interval between surgery for RCC and lung mass detection. LC histology resulted adenocarcinoma in 4 cases and large cell carcinoma in 1 case and no small cell carcinoma was discovered. Conclusions: A non-negligible proportion of lung masses diagnosed after surgery for RCC are not caused by systemic progression but do represent an independent biologic phenomenon. Given the key differences in therapeutic strategy, a precise differential diagnosis based on histological characterization is mandatory. Further investigations are required to validate the best predictors to differentiate LC from RCCM+. SOURCE OF Funding: None