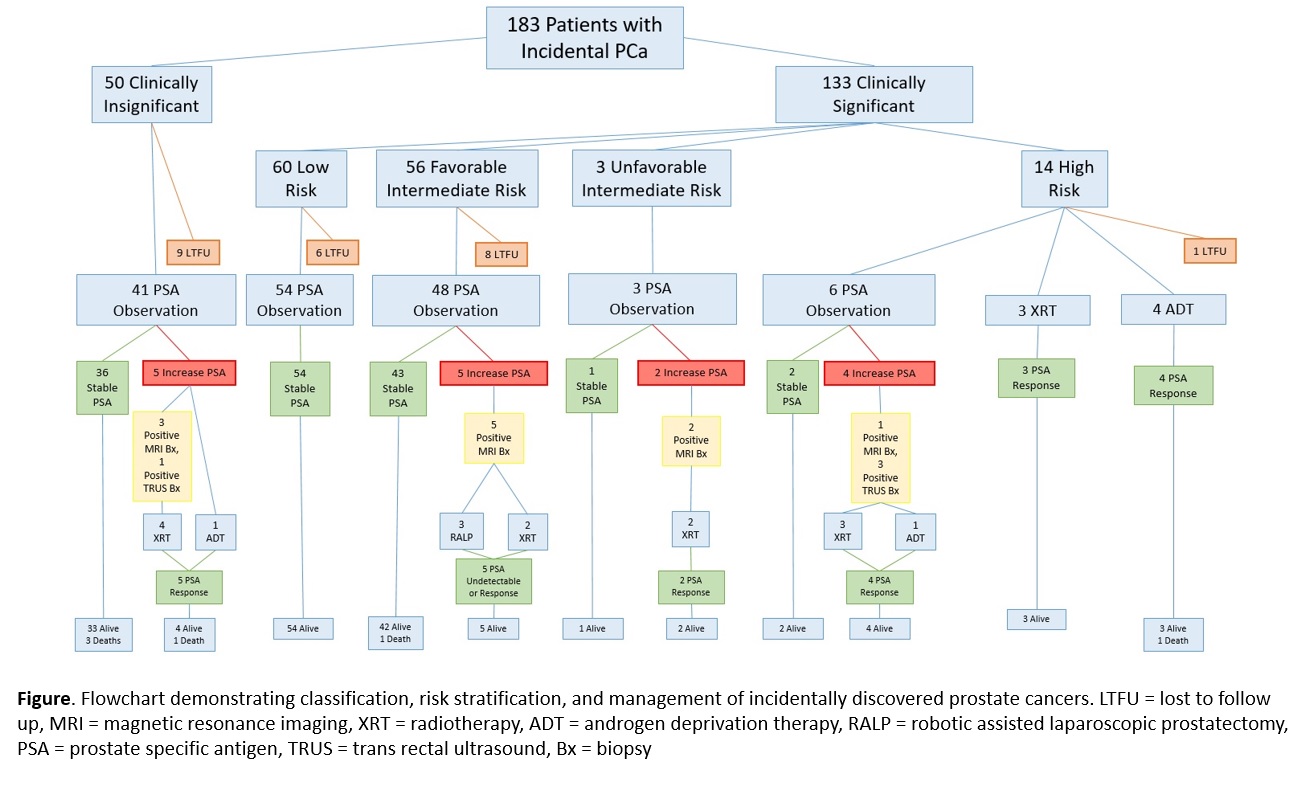
Introduction: Rates of incidental prostate cancer (iPCa) after Holmium Laser Enucleation of the Prostate (HoLEP) are higher than in other bladder outlet surgeries. Management presents a challenge considering the effects of HoLEP on anatomy and other causes of mortality in the older population. We examined cancer characteristics and initial management of patients with iPCa after HoLEP to understand the significance of these incidentally discovered cancers. Methods: Patients with iPCa were identified over a 4 year period from a prospectively maintained institutional database. Clinical data collected included preoperative PSA levels, cancer stage, grade, initial management, post operative PSA, staging imaging or biopsy. We defined clinically significant cancers as those where treatment other than watchful waiting was recommended by NCCN guidelines based on predicted life expectancy, which was estimated using the Social Security Life Expectancy Calculator. Results: 183/913 (20%) patients were diagnosed iPCa after HoLEP. 133 patients (73%) had clinically significant and 50 patients (27%) had clinically insignificant iPCa. Of clinically significant cancers, 7 patients with high risk PCa were managed with upfront local treatment and the rest underwent PSA surveillance (Figure). 11 experienced a PSA increase and underwent local treatment after confirmatory biopsy: 3 underwent RALP, 7 underwent XRT and one underwent ADT, all with appropriate PSA response to treatment. The clinically insignificant population underwent PSA observation. 9 were lost to follow up and 5 experienced a PSA increase triggering intervention: 4 underwent XRT and 1 underwent ADT with appropriate PSA response. At a mean follow-up of 16.3 months (IQR 7.9 – 13.4 months), there were 6 deaths, all from non-cancer related causes. Conclusions: Despite the low risk nature of many post-HoLEP iPCA, the majority were classified as clinically significant cancers based on NCCN guidelines. Data driven guidelines for pre-operative screening evaluation and post-operative management of iPCa after HoLEP are critical given the frequency and clinical implications these cancer diagnoses. SOURCE OF Funding: None

 photo")