Session: PD29: Bladder Cancer: Epidemiology & Evaluation II
PD29-04: PREDICTORS OF DEEP INCISIONAL AND ORGAN/SPACE SURGICAL SITE INFECTION FOLLOWING RADICAL CYSTECTOMY: RESULTS FROM THE ACS NSQIP SURGICAL REGISTRY
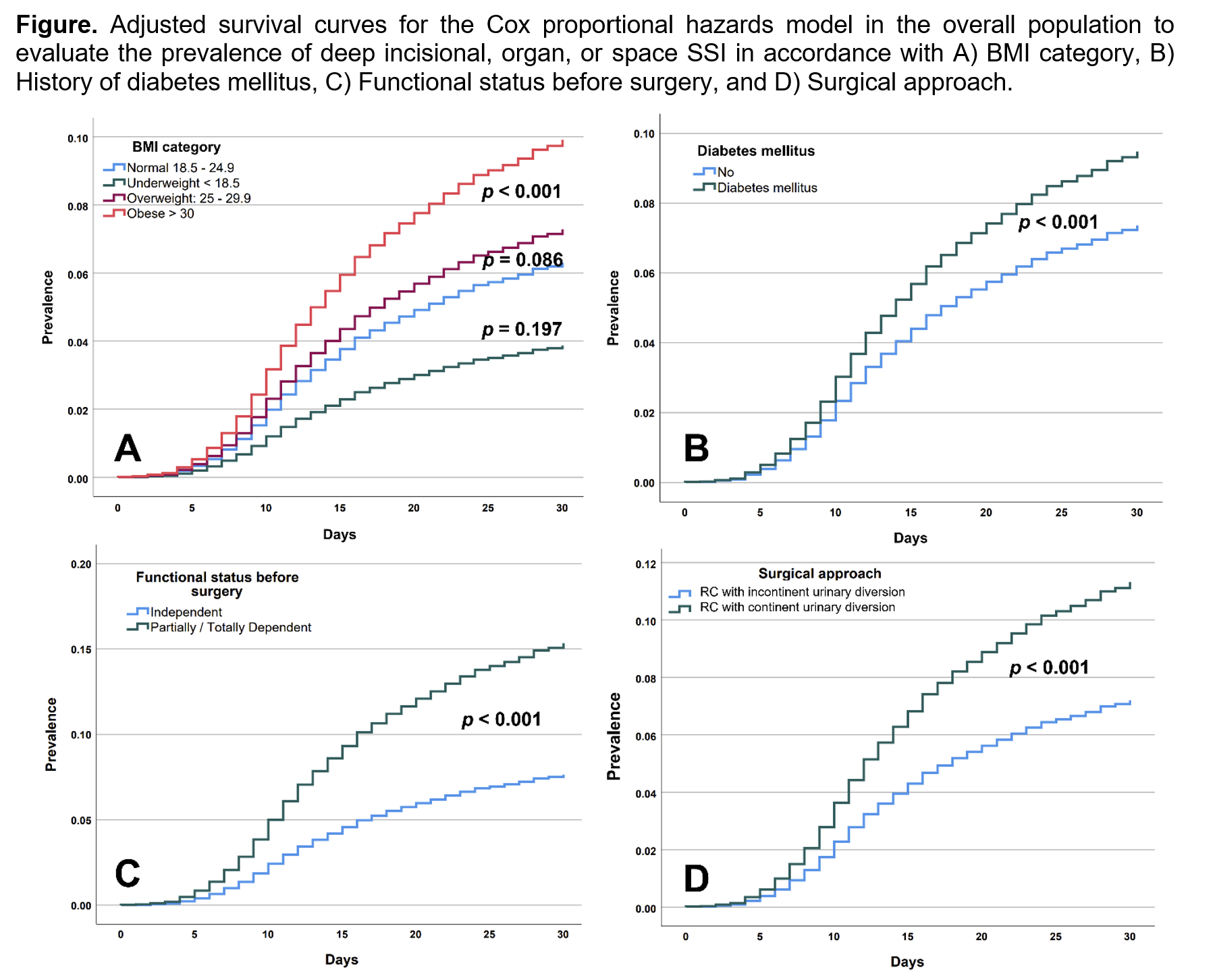
Introduction: Radical cystectomy (RC) with urinary diversion is the standard treatment for muscle-invasive and persistent high-risk treatment-refractory non–muscle-invasive bladder cancer. Surgical site infection (SSI) is a serious postoperative complication following RC. The objective of this study is to evaluate clinical risk factors associated with postoperative deep incisional or organ/space SSIs following RC in a contemporary cohort of patients using the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) surgical registry Methods: Using the ACS NSQIP surgical registry from 2015-2020, we selected patients =18 years that had the diagnosis of bladder cancer and underwent RC with incontinent urinary diversion (ileal conduit) or RC with continent urinary diversion. Clinical, demographic, type of surgical approach, and reports of 30-day postoperative deep incisional or organ/space SSIs were assessed. Statistical analysis was performed with SPSS v.28. A p-value <0.05 was considered statistically significant. Results: A total of 13,081 patients were analyzed, 1,061 (8.1%) with deep incisional or organ/space SSI. Of these patients, 11,021 (84.3%) patients underwent RC with incontinent urinary diversion and 2,060 (15.7%) underwent continent urinary diversion. Overall, 10,696 (81.8%) patients were male, age was 69 ± 9.7 years, BMI was 28.5 ± 5.7 kg/m2, diabetes mellitus prevalence was 2,534 (19.4%), and patients classified as functionally independent before surgery was 12,858 (98.3%). On multivariable-adjusted Cox regression analysis, presence of obesity (HR = 1.60, 95% CI: 1.35 - 1.90), diabetes mellitus (HR = 1.30, 95% CI: 1.13 - 1.51), being partially or totally dependent before surgery (HR = 2.09, 95% CI: 1.44 - 3.03), and RC with continent urinary diversion approach (HR = 1.61, 95% CI: 1.38 - 1.88) were associated with a higher risk of deep incisional or organ/space SSI postoperatively. (Figure) Conclusions: Patients with obesity, diabetes mellitus, functional dependence before surgery, or those who underwent RC with a continent urinary diversion approach have a higher risk of developing postoperative deep incisional or organ/space SSIs following RC. SOURCE OF Funding: No