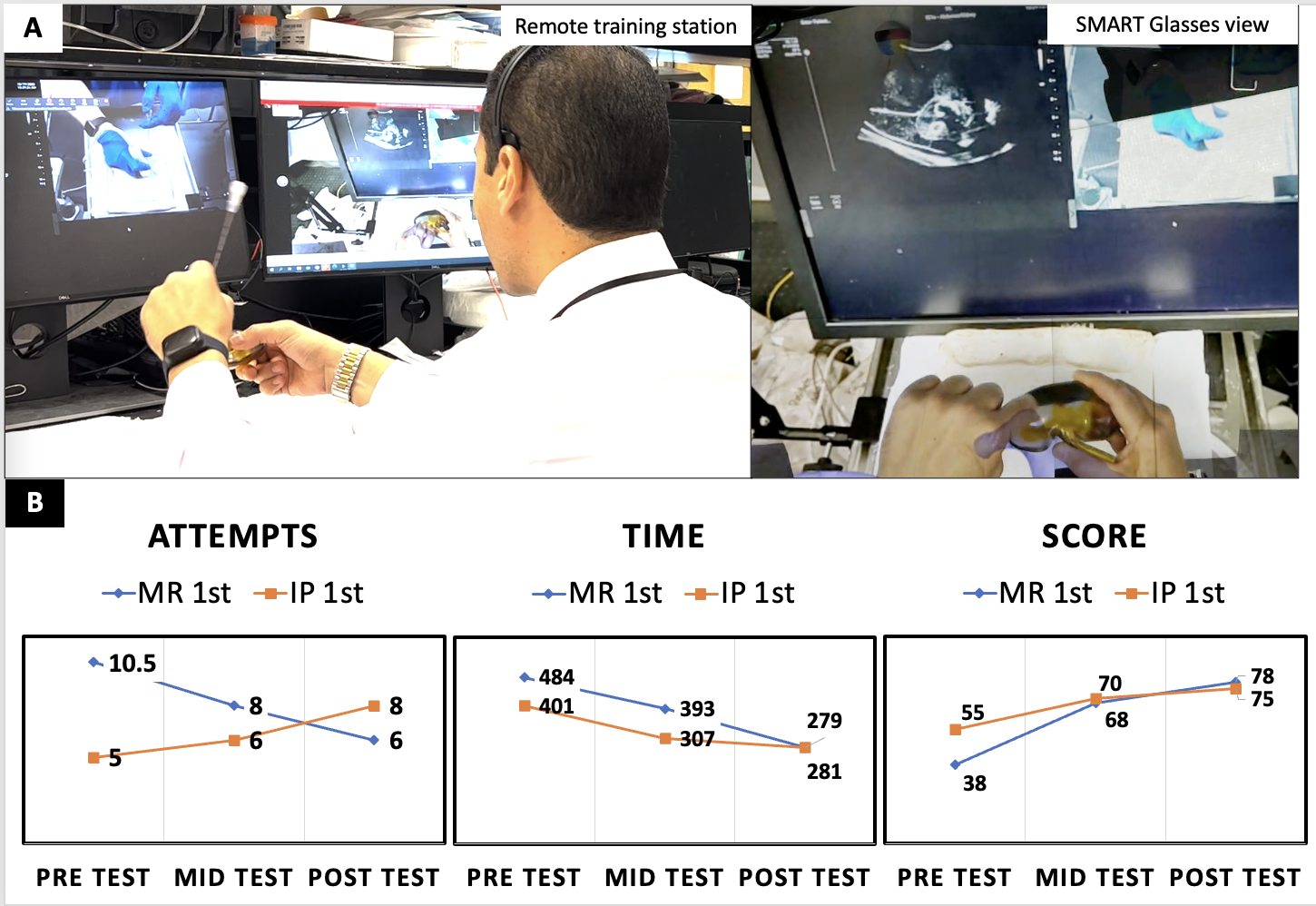
Introduction: MR enables the fusion of two world view video streams allowing an overlay of an instructor’s hands into the trainee’s view in real time. We aim to evaluate remote MR training compared to in-person (IP) training using a validated US-guided percutaneous renal access hydrogel simulation model. Methods: 12 residents with <5 cases were randomized into 2 groups. Anatomy and US-guided percutaneous access (PCA) steps were reviewed by trainees prior to completing a (1) pre-test, (2) training session (either MR or IP), (3) mid-test, (4) crossover training and (5) final post-test. Groups were randomized to MR vs IP training first where faculty guided trainees through PCA on a standard hydrogel model. During MR training faculty guided trainees wearing SMART glasses (Vuzix M4000) that transmitted audio and the merged surgical field (Fig 1a). In all 3 tests trainees independently gained needle access, guidewire passage and serial dilatation of the lower and upper pole. Number of attempts, time and 2 reviewers’ scores of each session using a validated grading tool were collected. Post-training surveys evaluated trainee perceptions. Results: On the pre-test, IP group had a higher average score compared to the MR group (55 vs 38, p=0.02) and less average access attempts (5.4 vs 10.5, p<0.05) with comparable times (484 s vs 401, p=0.18). Comparing pre to mid tests, MR vs IP showed a greater improvement in PCA attempts by 22.9% vs 7.4% (p=0.13), time by 19.5% vs 17.9% (p=0.39) and score by 65% vs 25% (p=0.04). After cross-over training, only MR group improved in PCA attempts (14.9%), time (17%) and score (7%). Comparing pre to post-tests the MR 1st vs IP 1st group showed a greater improvement in PCA time (24% vs 14%, p=0.23) and score (39% vs 16%, p=0.03) (Fig 1b). 66.7% of trainees found MR training to be similar to IP regarding usefulness, clarity, accuracy, timeliness and quantity but only 8.3% preferring MR to IP. Participants reported similar confidence in ability to perform simulated US-guided renal access. Conclusions: Remote training using MR technology provided comparable learning to IP simulation training. Despite the improved performance and equivalent delivery when using MR technology, trainee perceptions towards remote training remain skeptical. SOURCE OF Funding: SAU education grant