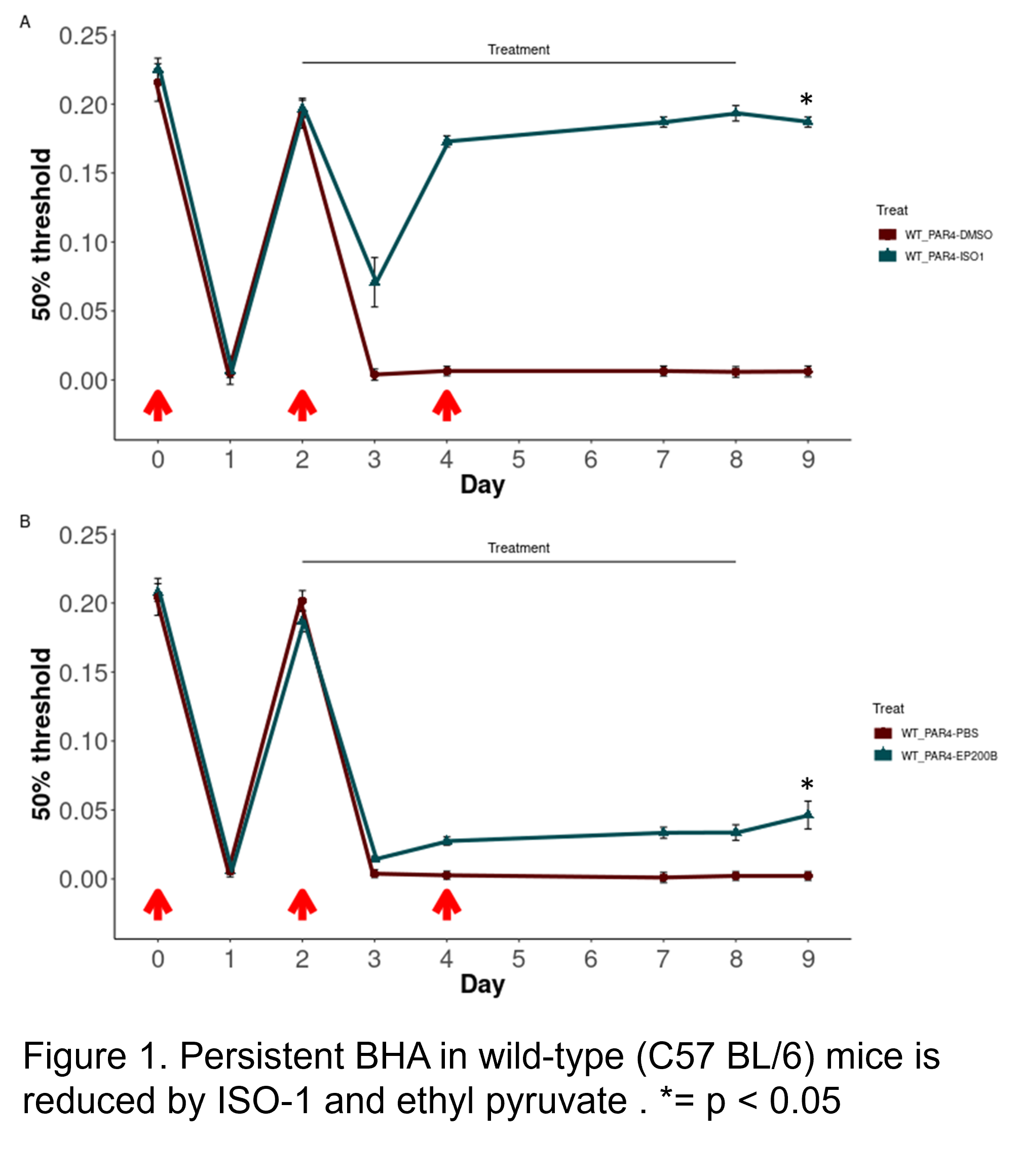
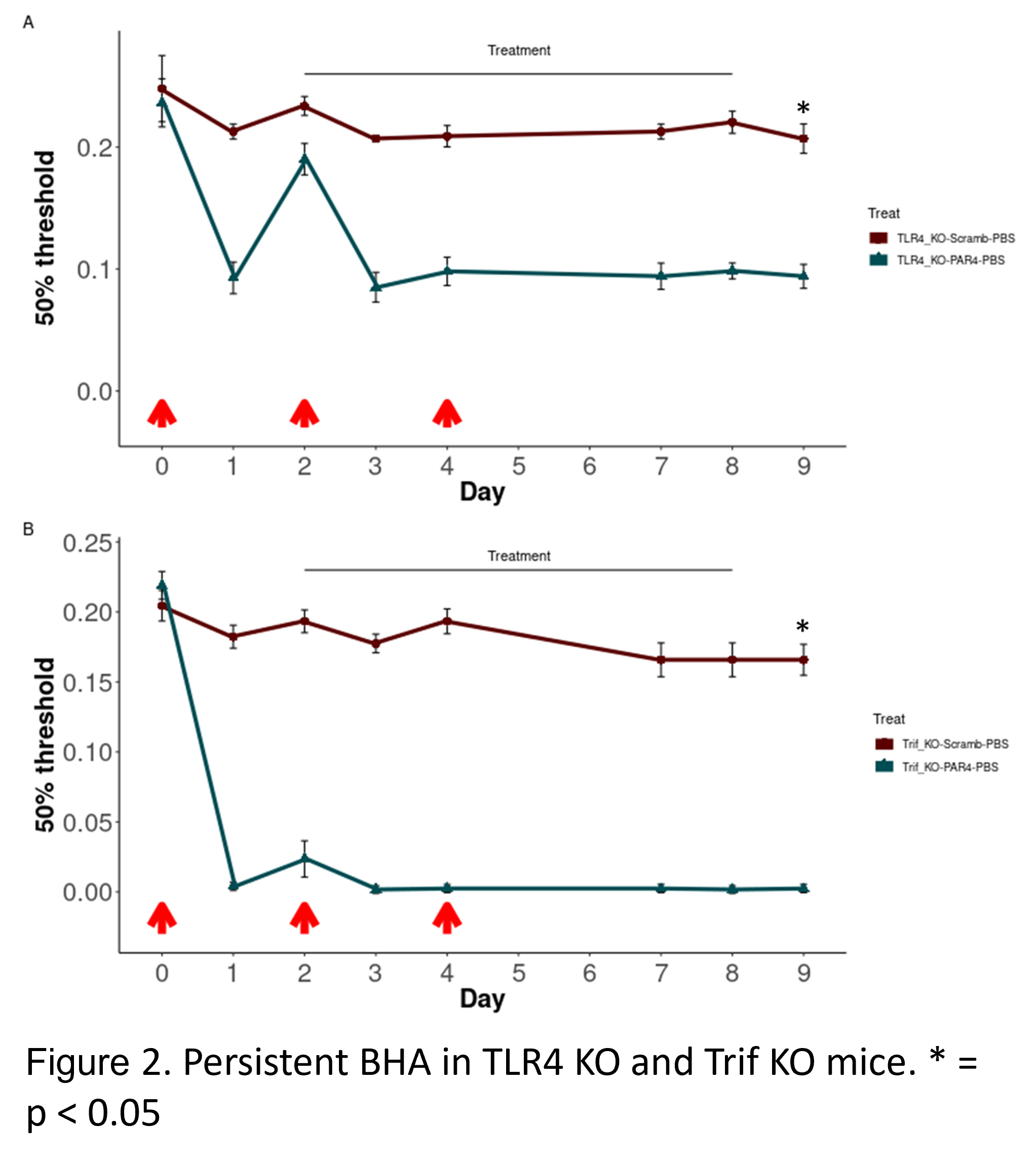
Introduction: Interstitial cystitis/Bladder pain syndrome is a painful condition with unknown etiology. Repeated intravesical PAR4 induced persistent bladder hyperalgesia (BHA) in mice that lasts several days after the last stimulus with little or no evidence of bladder inflammation. Our studies showed that spinal macrophage migration inhibitory factor (MIF) and High Mobility Group Box 1 (HMGB1) are critical causative factors. We aimed to dissect this persistent pain pathway and explore effective targets for treating persistent bladder pain. Methods: Persistent BHA was induced in female mice (WT, TLR4 null, Trif null) by three intravesical instillations (days 0, 2 and 4) with PAR4 agonist (100 uM; 1hr, scrambled peptide as control) under anesthesia. Lower abdominal hypersensitivity was measured by von Frey filaments on days 0-4 and 7-9. Intraperitoneal treatment was performed on days 2-8 and included: ISO-1 (MIF antagonist); 10% DMSO; ethyl pyruvate (EP; inhibits HMGB1 release); and PBS. Awake micturition parameters (voided volume; frequency) were assessed on day 9. Bladder histology assessed inflammation/edema. R was used for all analyses. Results: Inhibition of MIF activity with ISO-1 robustly reversed the PAR4-induced persistent BHA in WT mice (Fig 1A) while treatment with EP partially reduced BHA (Fig 1B). TLR4 deficiency substantially damped persistent pain (Fig 2A) while lack of Trif did not affect PAR4-induced persistent BHA (Fig 2B). No significant effects were noted on micturition volume, frequency, inflammation, or edema. Conclusions: MIF, HMGB1, and TLR4 signaling activation are required for PAR4-induced persistent BHA. However, Trif may not be critical for persistent bladder pain. Further dissecting TLR4 downstream signaling pathway is necessary to identify important mediators and whether they act centrally or peripherally. This may lead to the discovery of novel potential therapeutic targets to treat persistent bladder pain. SOURCE OF Funding: DK121695