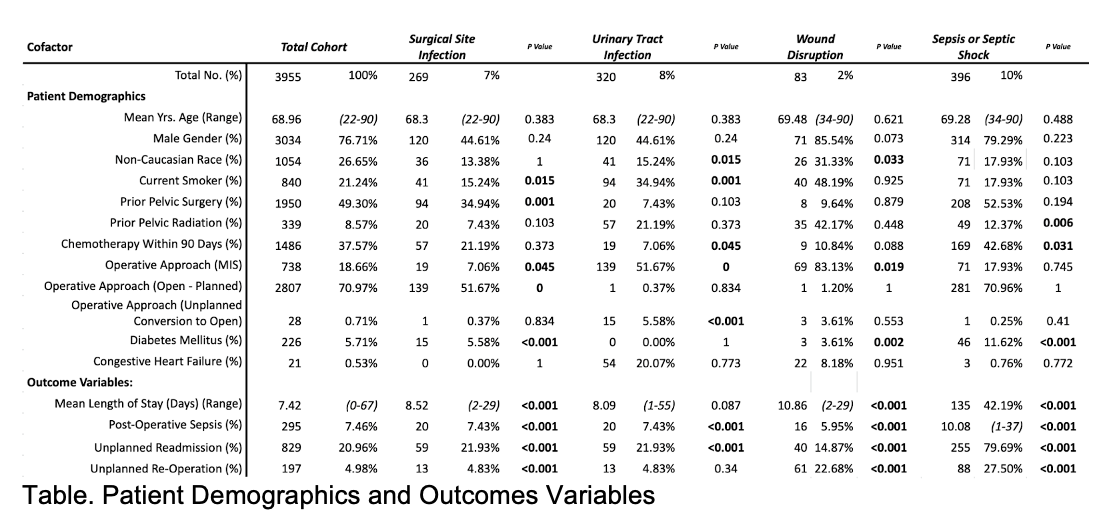
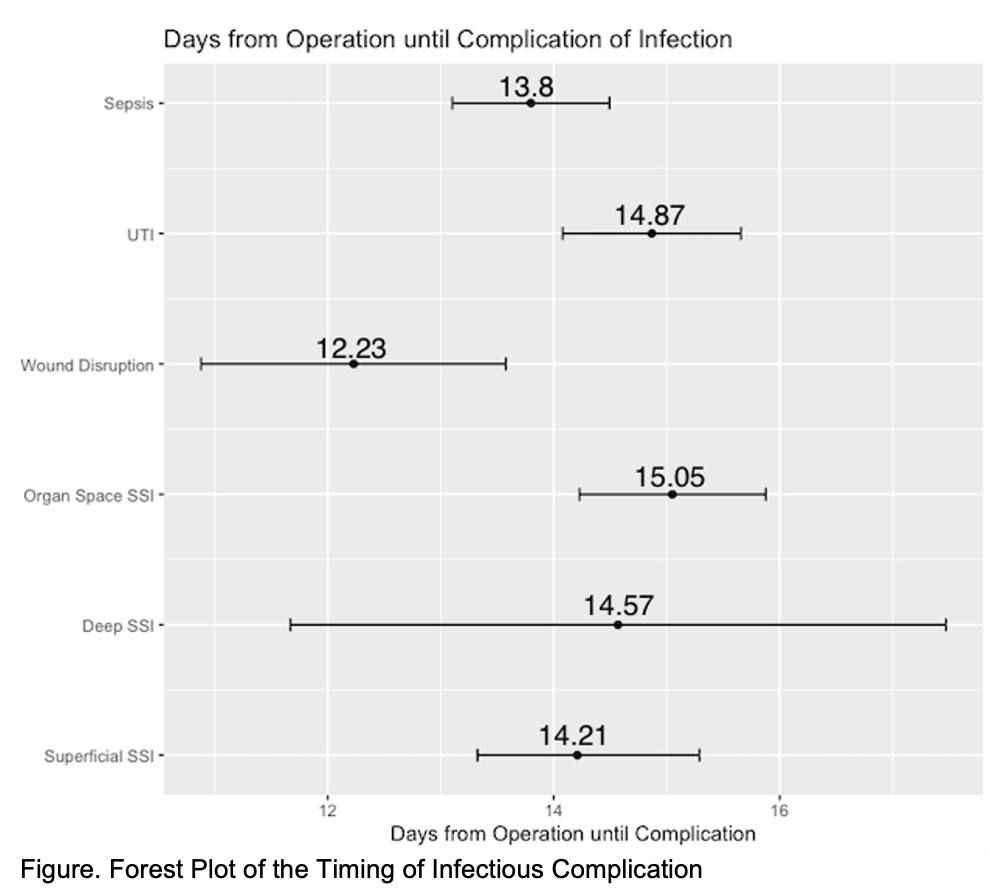
Introduction: Radical cystectomy (RC) with urinary diversion is the primary treatment option for muscle invasive bladder cancer (MIBC) and select patients for non-muscle invasive bladder cancer (NMIBC). Surgical and non-surgical Infection after RC is a devastating complication. Postoperative infection has been shown to increase admission to ICU, increase length of hospital stay, increased readmission and double the mortality rate. We aim to add to the literature of the characteristics, timing, and predilection of infection after RC. Methods: The ACS NSQIP is a health insurance portability and accountability act (HIPAA) compliant data file containing patient cases from 706 participating hospital institutions. This retrospective study focused on radical cystectomy cases in the NSQIP data set for bladder cancer. Patients with missing data or had multiple infections were excluded. The patients were then subgrouped to surgical site infection (SSI), wound disruption, UTI, and sepsis (sepsis and septic shock). Results: Among the 3955 patients, the rate of SSI, UTI, wound disruption, sepsis/septic shock was 11.9%, 8.1%, 2.1%, and 10.0% (Table). The average days from operation until infectious complications were 15.1 days for organ space SSI, 14.57 days for deep SSI, 14.2 days for superficial SSI, 14.9 days for UTI, 12.2 days for wound disruption, and 13.8 days for sepsis (figure). Multivariable analysis for all infections identified diabetes as an independent variable associated with SSI (p=0.003), UTI (p=0.039), and sepsis/septic shock (p < 0.001). Prior pelvic radiation was associated with SSI (p=0.001) and sepsis/septic shock (p=0.012). Furthermore, all infectious etiologies were associated with readmission on multivariable regression. Conclusions: Infection after radical cystectomy can be an often a serious complication. We identified that the timing of wound disruption to occur earliest while organ space SSI was identified late. Diabetes was associated with all the infectious complications while prior radiation was associated with SSI and sepsis. SOURCE OF Funding: n/a