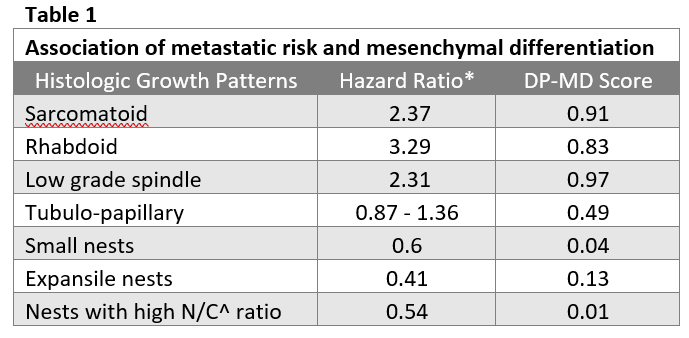
Introduction: Epithelial-to-mesenchymal transition (EMT) results in poor prognosis sarcomatoid and rhabdoid histologic growth patterns (HGP) of ccRCC. However, only ~15% of metastatic cases reveal areas of sarcomatoid/rhabdoid differentiation in the primary tumor. We questioned whether a computer can learn salient features of EMT that are associated with risk of metastatic progression across all HGPs of ccRCC. Methods: The project uses 410 digital H&E slides of ccRCC. We incorporated a novel co-training approach into a machine learning model (MLM) and trained the model to distinguish epithelial (nested) and mesenchymal (sarcomatoid, rhabdoid) HGPs in a Utah cohort. The trained MLM is applied to the TCGA KIRC cohort (n=360) with annotated regions of nested, tubulo-papillary, low grade-spindle, sarcomatoid and rhabdoid HGPs for which the hazard ration of metastatic progression was published. For each case, the MLM outputs a mesenchymal-differentiation (DP-MD) score on a scale of 0 to 1 where closer to 1 is higher likelihood of EMT. Results: A unique machine learning / AI model was developed to quantify sarcomatoid differentiation in ccRCC with no obvious histologic signs of mesenchymal morphology. H&E stains were used as separate inputs of a contrastive co-training model (H/E-CCTM) to force the learning of mesenchymal features. The inclusion of a semi-supervised learning component improved the accuracy of predicting mesenchymal differentiation by > 4% over other state-of-the-art co-training algorithms and performed equally well when trained on 10% versus 100% of labeled cancer data. Sarcomatoid, low grade spindle and rhabdoid cases received average DP-MD scores of 0.91, 0.97 and 0.83, respectively in a held-out test set, while cases with nested morphology, including expansile, and high nuclear to cytoplasmic ratio averaged DP-MD scores of 0.08. Tubulo-papillary HGPs without obvious mesenchymal features obtained an average DP-MD score of 0.49. Conclusions: Computer-assisted morphometric analysis can be used to quantify mesenchymal differentiation and has the potential to improve the prediction of metastatic risk in ccRCC and the selection of patients for adjuvant treatment after nephrectomy. SOURCE OF Funding: Huntsman Cancer Foundation, NIH P30CA042014