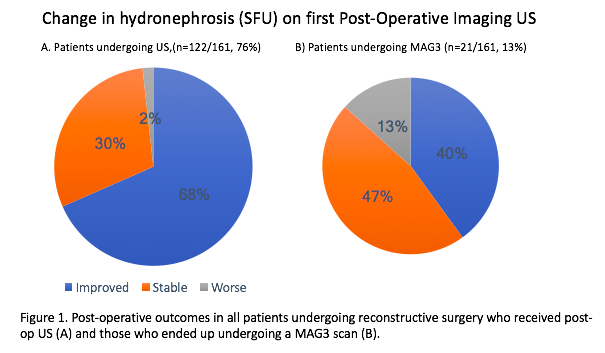
Introduction: Upper tract obstruction can present with flank pain, infections, hematuria, and impaired kidney function. The gold standard for evaluation of obstruction is a MAG3 nuclear renal scan. There is no consensus however on optimal post-operative imaging surveillance strategy. Studies have demonstrated that renal ultrasound (US) may be an effective substitute modality that is quick, easily accessible, low cost, and avoids risks of invasiveness, radiation exposure, and infection. To our knowledge, prior studies collected both US and MAG3 to compare effectiveness. This is the first data of real world surveillance of post-upper tract reconstruction with US. Methods: Retrospective analysis of an institutional database on reconstructive urologic surgery. Clinical variables were collected through electronic medical record review. Descriptive statistics were used to assess presence of and change in preoperative hydronephrosis, need for MAG3, obstruction, and reintervention. Results: 161 patients underwent upper tract reconstruction over a 6 year period. There was missing data for 29 patients. Overall, success defined by no obstruction on MAG3 was 96%. Pre-op, 3 patients (1.8%) had SFU 0, 19 (12%) SFU 1, 55 (34%) SFU 2, 58 (36%) SFU 3, 28 (17%) SFU 4, 5 (3.1%) had missing data, and 2 (1.2%) had a fistula. First imaging was obtained after surgery at a median (IQR) of 126.5 days (84-154). Post-op, 78 patients (48%) had improved hydronephrosis, 34 (21%) were stable, 2 (1.2%) were worse, and 47 (29%) had missing data. Of the 21 patients who underwent MAG3 studies, 6 (29%) had improved hydronephrosis, 7 (33%) were stable, 2 (10%) were worse. Only 2 patients were obstructed on MAG3. Two patients underwent stenting, 2 had PCN, and 1 had reconstructive surgery. Not all interventions were failures (i.e., placed for an infection). Conclusions: Renal US is a safe and effective tool for surveillance after upper tract reconstruction. The majority of our patients avoided a MAG3 study, which may influence future practice patterns. SOURCE OF Funding: None

 photo")