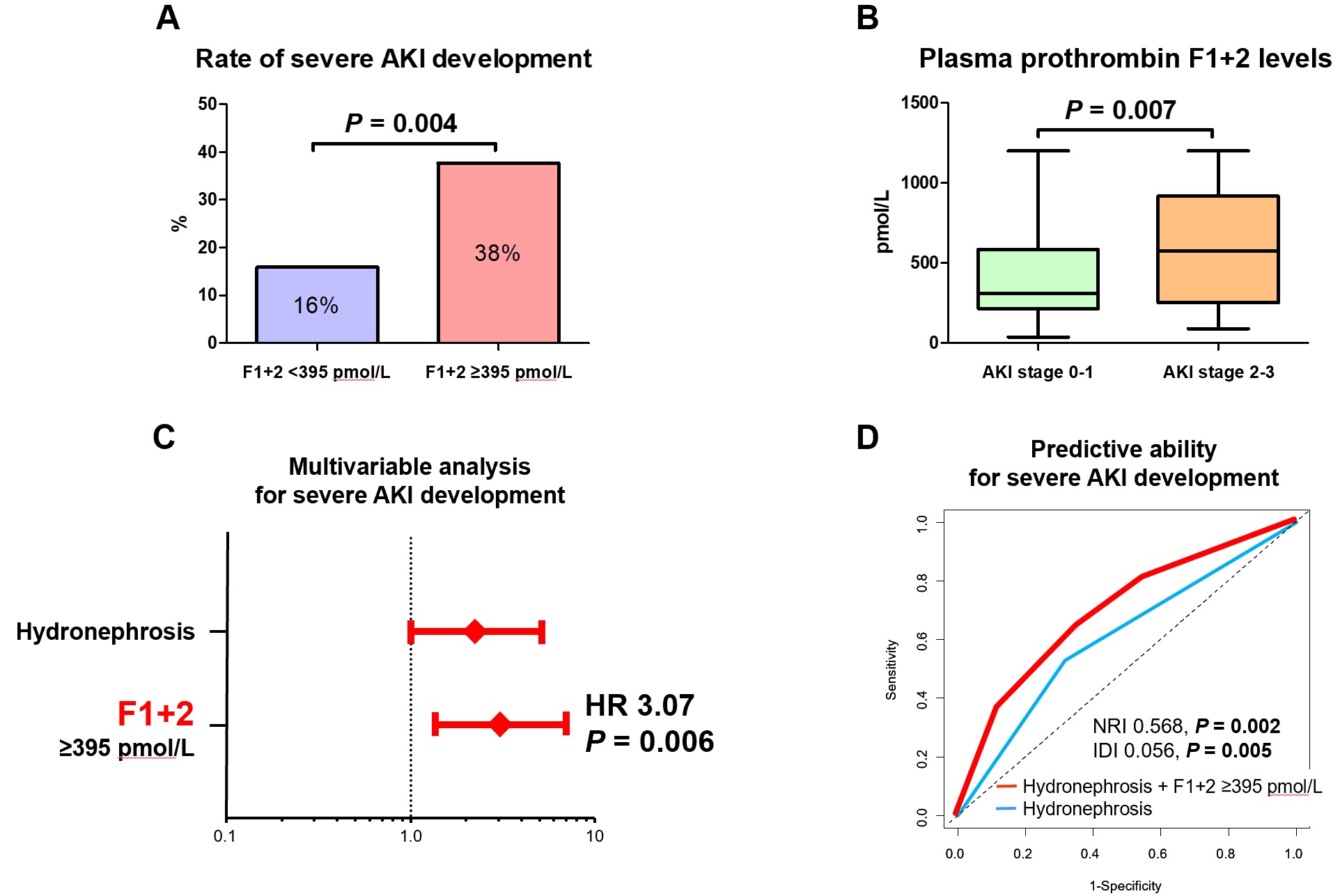
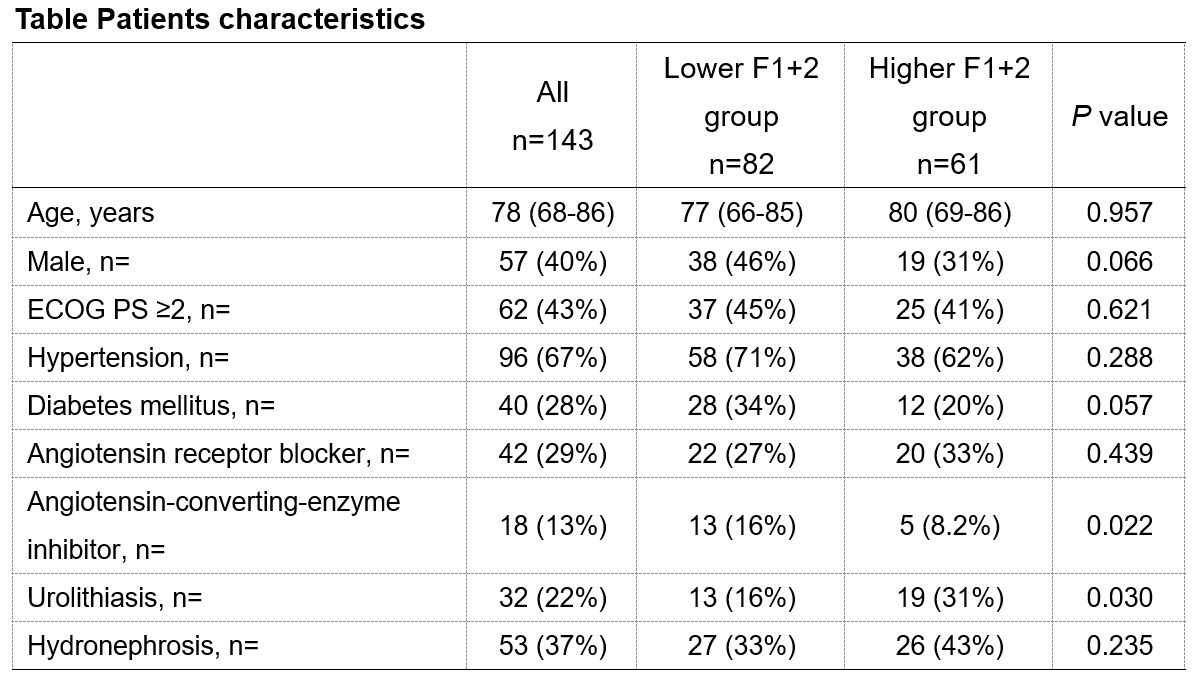
Introduction: Elevated prothrombin fragment 1+2 (F1+2), produced during conversion of prothrombin to thrombin, indicates excess thrombin production and serves as a molecular marker of activated coagulation. The aim of this study was to investigate the impact of elevated F1+2 on the development of severe acute kidney injury (AKI) in patients with urological sepsis. Methods: We prospectively collected the data from 143 patients with urological sepsis between March 2017 and March 2019. AKI was defined according to the KDIGO criteria. Patients were divided into two groups: lower F1+2 (plasma F1+2 levels <395 pmol/L) and higher F1+2 groups (plasma F1+2 levels =395 pmol/L). Multivariable logistic regression analysis was performed to evaluate the impact of elevated F1+2 on the severe AKI development. We evaluated predictive ability of elevated F1+2 for the severe AKI development using the receiver operating characteristic curve and compared using net reclassification improvement (NRI) and integrated discrimination improvement (IDI). Results: Median age was 78 years old in this cohort. Of 143 patients, 61 were classified as a higher F1+2 group and 36 developed to severe AKI (AKI stage 2-3). Rate of severe AKI development in the higher F1+2 group was significantly higher than that of the lower F1+2 group (Fig. A; P = 0.004). Plasma F1+2 levels in patients with severe AKI was significantly higher than that in patients with stage 0-1 AKI (Fig. B; P = 0.007). In multivariable analysis, plasma F1+2 level =395 pmol/L was selected as a significant independent risk factor for severe AKI development (Fig. 3; hazard ratio 3.067, P = 0.006). The predictive ability of hydronephrosis plus elevated F1+2 levels for severe AKI development was significantly improved compared with hydronephrosis alone (Fig. D). Conclusions: Elevated prothrombin F1+2 is a risk factor of severe AKI in patients with urological sepsis. SOURCE OF Funding: None