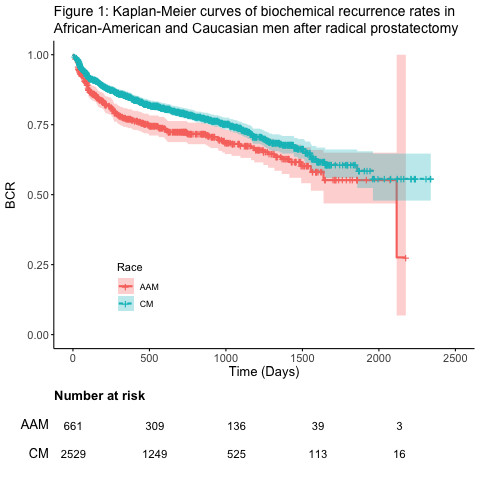
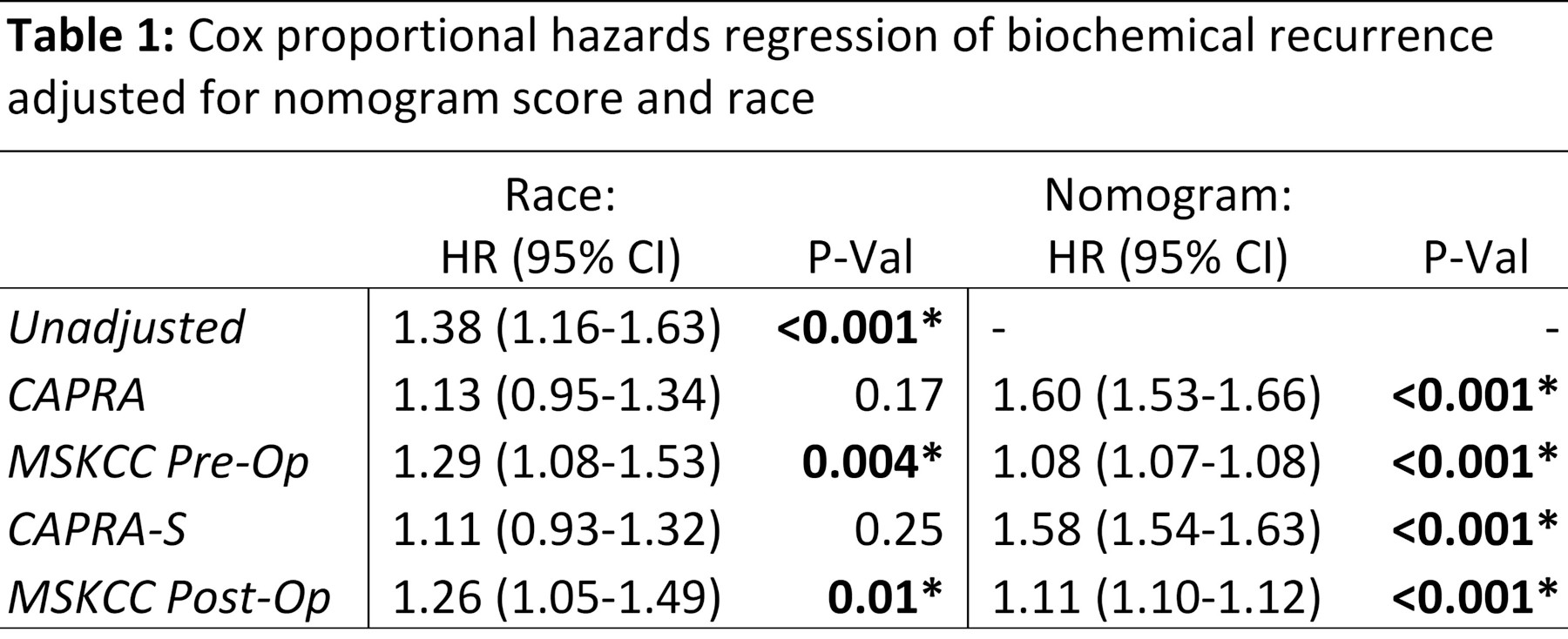
Introduction: This study aims to determine if there is a difference in prostate cancer nomogram-adjusted risk of biochemical recurrence (BCR) and/or adverse pathology (AP) between African American (AAM) and Caucasian men (CM) undergoing radical prostatectomy (RP). Methods: A retrospective review was performed of men undergoing RP in the Pennsylvania Urologic Regional Collaborative (PURC) between 2015-2021. Cox proportional hazards regression models were used to compare the rate of BCR after RP, and logistic regression models were used to compare rates of AP after RP between CM and AAM adjusting for the CAPRA, CAPRA-S, and MSKCC pre- and post-operative nomogram scores. Results: Rates of BCR and AP after RP were analyzed from 3,190 and 5,029 men meeting inclusion criteria. The 2-year BCR free survival was lower in AAM (72.5%) compared to Caucasian men (CM) (79.0%), with a hazard ratio (HR) of 1.38 (95% CI 1.16-1.63, p<0.001), demonstrated in Figure 1. The rate of BCR was significantly greater in AAM compared to CM after adjustment for MSKCC pre-op (HR 1.29; 95% CI 1.08-1.53; p=0.004), and post-op nomograms (HR 1.26; 95% CI 1.05-1.49; p<0.001) (Table 1). There was a trend towards higher BCR rates among AAM after adjustment for CAPRA (HR 1.13; 95% CI 0.95-1.35; p=0.17) and CAPRA-S nomograms (HR 1.11; 95% 0.93-1.32; p=0.25), which did not reach statistical significance. The overall rate of AP was similar between AAM (38.4%) and CM (37.8%) (OR 1.02; 95% CI 0.89-1.17; p=0.72) but was significantly greater in AAM compared to CM after adjusting for CAPRA (OR 1.28; 95% CI 1.10-1.50; p=0.001) and MSKCC nomograms (OR 1.23; 95% CI 1.06-1.43; p=0.007). Conclusions: This analysis of a large multicenter cohort provides further evidence that AAM may have higher rates of BCR and AP after RP than is predicted by CAPRA and MSKCC nomograms. Accordingly, AAM may benefit with closer surveillance, and differently tailored thresholds in treatment protocols. SOURCE OF Funding: NA