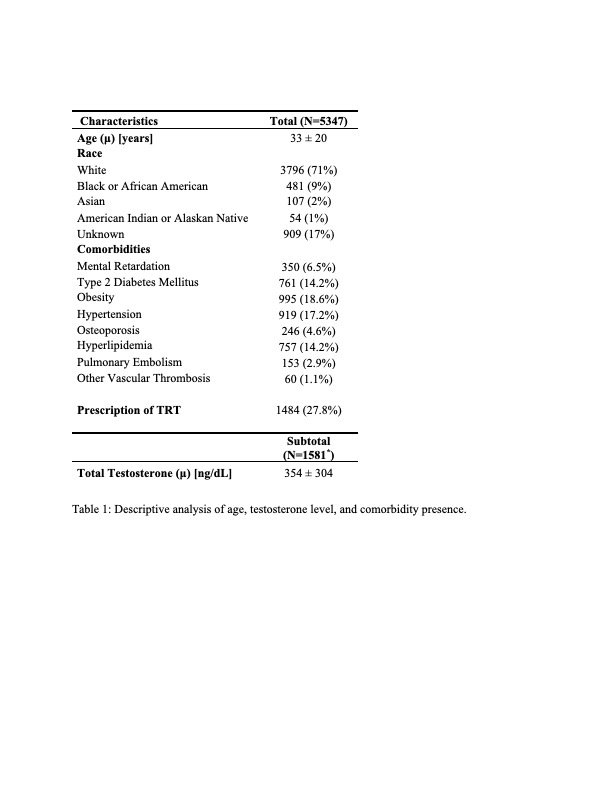
Introduction: Klinefelter Syndrome (KS, 47 XXY) represents the most common genetic form of male hypogonadism. Given the degree and prevalence of hypogonadism in these men, it is recommended that patients with KS and testosterone deficiency should be treated with lifelong testosterone supplementation (TRT) that begins at puberty to secure the development of sexual male characteristics and prevent long-term sequelae. Primary hypogonadism (including KS) is an on-label indication for TRT. The objective of this study was to determine the rates of hypogonadism and prescription of TRT in men with KS. We hypothesized that men with KS are under treated for testosterone deficiency with TRT because of the relationship between KS and neurocognitive impairment. Methods: We queried TriNetX, a large, multicenter electronic health record database, to identify all men with a diagnosis of Klinefelter syndrome (ICD-10-CM Q98.4). We collected data on comorbidities including cognitive impairment, type 2 diabetes mellitus, obesity, hyperlipidemia, hypertension, osteoporosis in addition to demographic characteristics. Prevalence of testosterone deficiency was determined as defined by testosterone level < 300 ng/dl. The primary outcome of the study was prescription of any of the following forms of TRT on the day of diagnosis or later. Results: There were 5,437 total men with diagnosis of KS. A total of 1,581 men with KS received laboratory measurement of testosterone level, 1,113 (70.4%) of whom were hypogonadal. Mean testosterone level in this group was 354 ng/dL [50 – 658]. Of the 1,113 men found to be hypogonadal, only 657 (59.0%) men were given prescription for TRT. Conclusions: Despite the recent addition of KS as an indication for treatment to the FDA-approved label for TRT, in this large, retrospective study, TRT was under-prescribed in men with KS. Under treatment of hypogonadism in men with KS can lead to long-term consequences such as metabolic syndrome and cognitive impairment. This is the first study to evaluate TRT prescribing patterns in men with KS. Future research is needed to corroborate these findings and to evaluate barriers, especially as related to to receiving care in this population. SOURCE OF Funding: This work was supported by NIH Grant R01 DK130991 and Clinician Scientist Development Grant from the ACS to Ranjith Ramasamy

 photo")