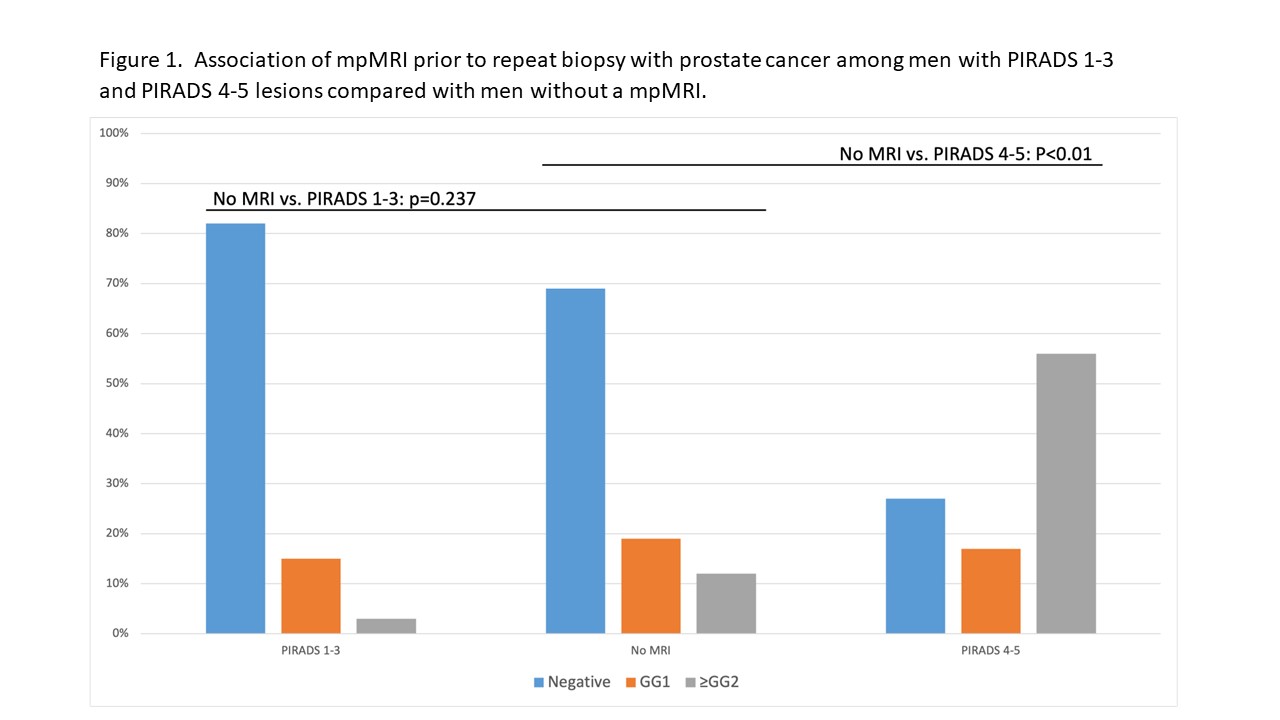
Introduction: High-grade prostatic intraepithelial neoplasia (HGPIN) and atypical small acinar proliferation (ASAP) are associated with an increased risk of clinically significant prostate cancer (CaP) on subsequent prostate biopsy. We investigated the association of multiparametric MRI (mpMRI) findings in men with a previous diagnosis of HGPIN or ASAP with findings on repeat biopsy. Methods: We retrospectively reviewed patients with multifocal HGPIN or ASAP undergoing a repeat biopsy in the Michigan Urological Surgery Improvement Collaborative (MUSIC) registry. We compared the proportion of men with a benign biopsy, GG1, and =GG2 CaP on repeat biopsy within 24 months of the initial biopsy with HGPIN/ASAP. Men were placed into three groups: 1) without a mpMRI, 2) with a mpMRI demonstrating a PIRADS 1-3 lesion, 4) and PIRADS 4-5 lesion. Men with a mpMRI performed before or after the initial biopsy that demonstrated HGPIN/ASAP were analyzed separately. Results: There were 219 men in the MUSIC registry with a diagnosis of HGPIN or ASAP on their initial biopsy that underwent a repeat biopsy, of which 86 had a mpMRI before (n=12) or after (n=74) the initial biopsy. Among men with a mpMRI after the initial biopsy (Figure 1), we noted that a lower proportion of men with PIRADS 1-3 lesions had GG1 (15%) or =GG2 (3.0%) CaP and a higher proportion had benign biopsies (82%) compared with men without a mpMRI (19%, 12%, and 70%, respectively, p=0.237). Men with a PIRADS 4-5 lesion after the initial biopsy had a higher proportion of =GG2 (56%) and GG1 (17%) CaP and a lower proportion of benign biopsies (27%) on repeat biopsy compared with men without a mpMRI (19%, 12%, and 70%, respectively, p<0.001). Among patients with a mpMRI prior to the initial biopsy, 0/12 patients were diagnosed with =GG2 CaP on repeat biopsy. Conclusions: Men with PIRADS 1-3 lesions on MRI after a diagnosis of HGPIN/ASAP had a low risk of clinically significant CaP on repeat biopsy while men with PIRADS 4-5 lesions were less likely to have benign biopsies and more likely to have clinically significant CaP compared with men without an MRI prior to repeat biopsy. MRI is a valuable tool to triage which men with HGPIN or ASAP on initial biopsy should undergo or avoid repeat biopsy without missing clinically significant CaP. SOURCE OF Funding: Blue Cross Blue Shield of Michigan, Rogel Cancer Center